
General Pathology — MCQs

On this page
A wedge-shaped area in the adrenal gland is affected. On histopathology, the nucleus is not seen but cellular outlines are intact. Which type of necrosis is being described?
Fat necrosis is not associated with which of the following procedures or conditions?
Congenital hypercoagulability states include all of the following EXCEPT:
Hemorrhagic infarction is seen in all except:
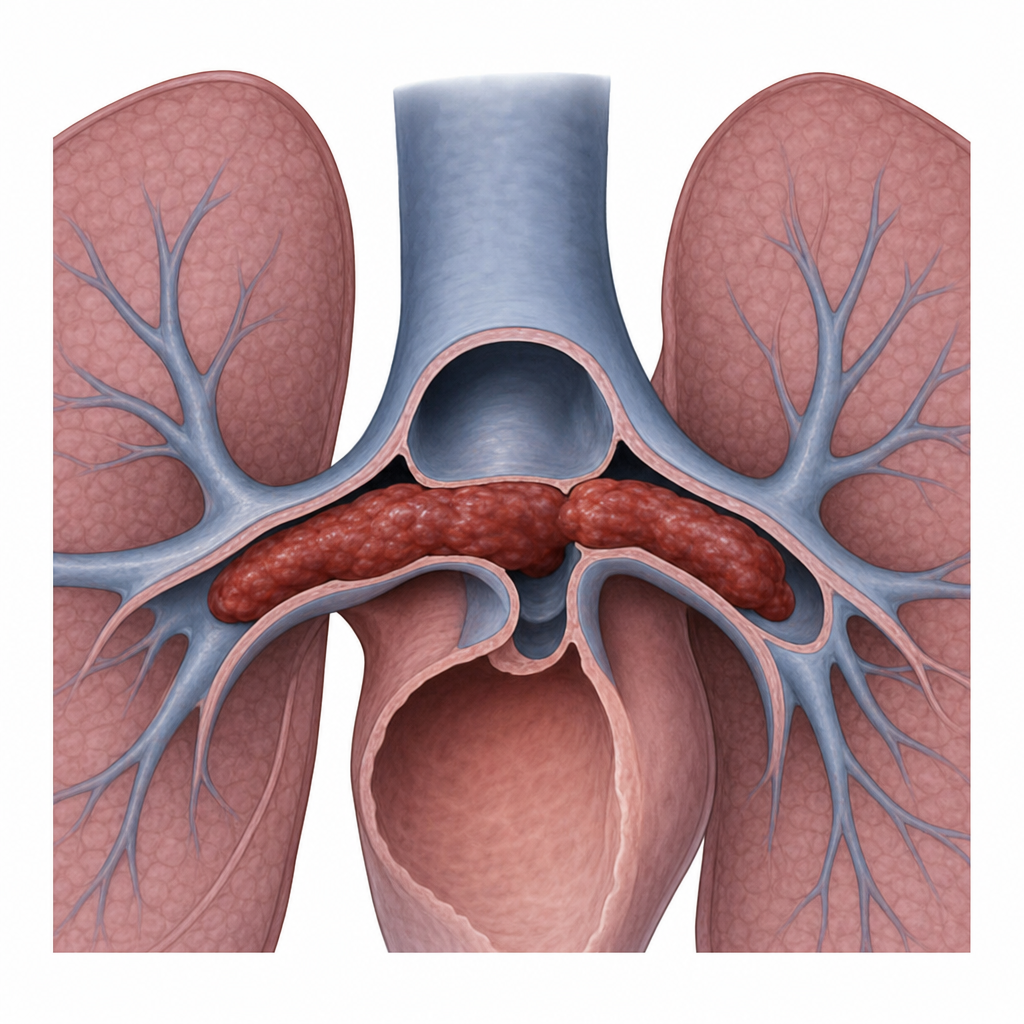
The embolus depicted in the cross-section is an example of which type?
Which of the following is NOT a mononuclear-macrophage?
Hemorrhagic infarction is seen in which of the following conditions?
A 60-year-old man presents with acute liver failure and undergoes successful orthotopic liver transplantation. For the first 3 days post-transplant, the graft exhibits poor function, characterized by minimal bile production. This poor graft function is attributed to reperfusion injury. Which of the following substances is the most likely cause of reperfusion injury in this transplanted liver?
All of the following are stress sensors/regulators for apoptosis, except?
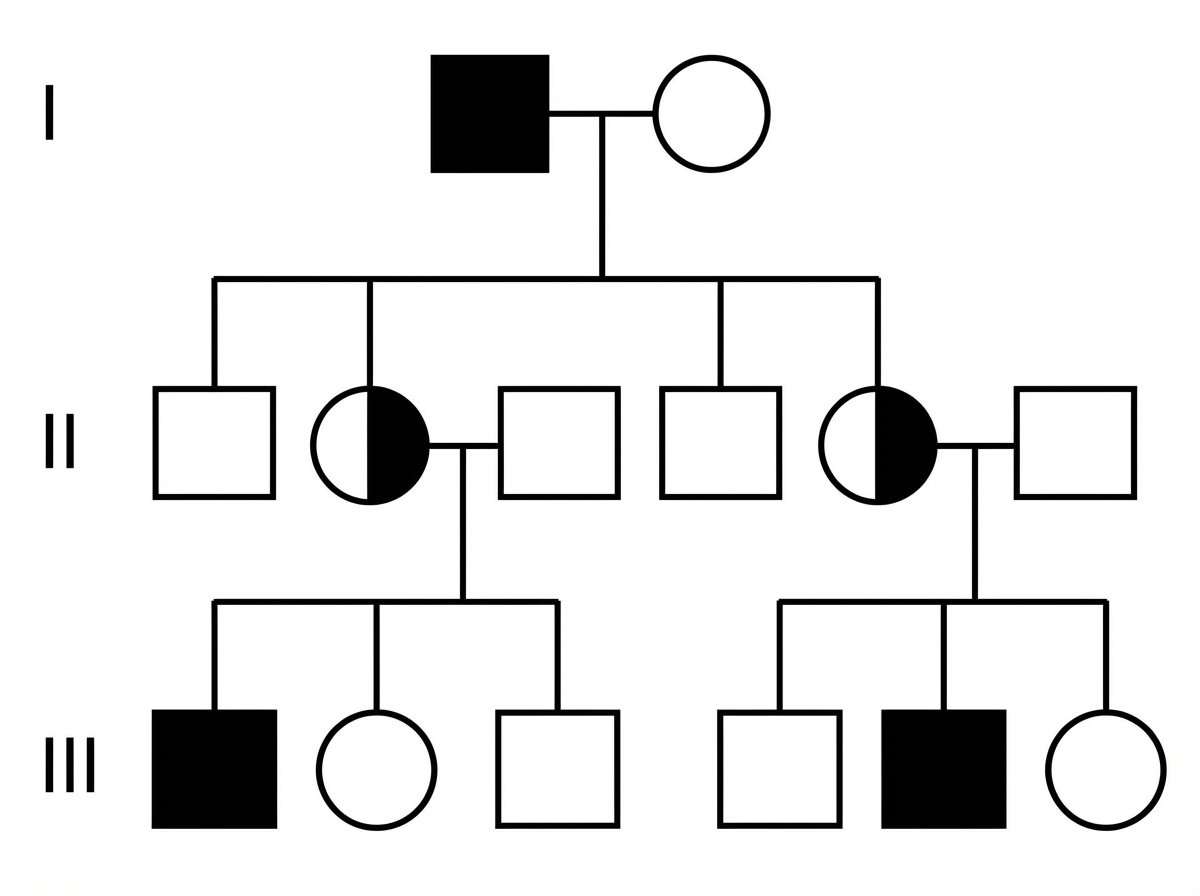
The given pedigree chart most appropriately resembles which of the following diseases?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app