
General Pathology — MCQs

On this page
Petechiae in scurvy is due to which of the following?
Malarial pigment is formed by?
Which of the following statements regarding lipofuscin is not true?
Conversion of normal cell into their tombstones is the hallmark of which type of necrosis?
Which of the following cell types is least sensitive to anoxia?
Pale infarct is seen in all of the following organs except?
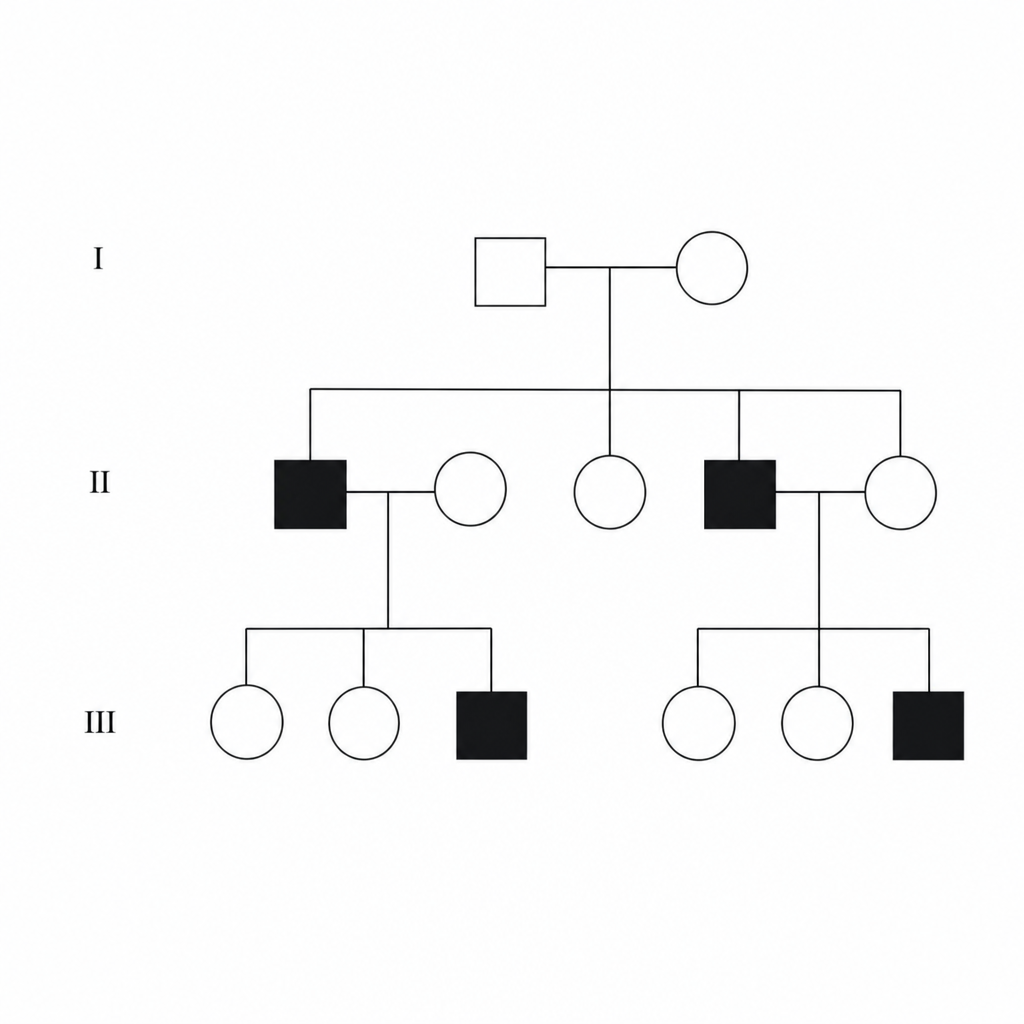
What is the pattern of inheritance shown in the given pedigree chart?
Which of the following acquired conditions is low risk for thrombosis?
Apoptosis causes all of the following except:
Which protein is implicated in Familial Amyloidosis?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app