
General Pathology — MCQs

On this page
Which of the following is NOT a transudate?
Which of the following best describes the initiation of apoptosis?
A 50-year-old woman, who underwent radical mastectomy and axillary node dissection for breast cancer one year ago, now notices her arm swells by the end of the day. What is the appropriate name for this fluid accumulation?
A patient with XO chromosomes and short stature is likely to have which of the following conditions?
Metaplasia is thought to be caused in most cases by:
Which organelle plays a pivotal role in apoptosis?
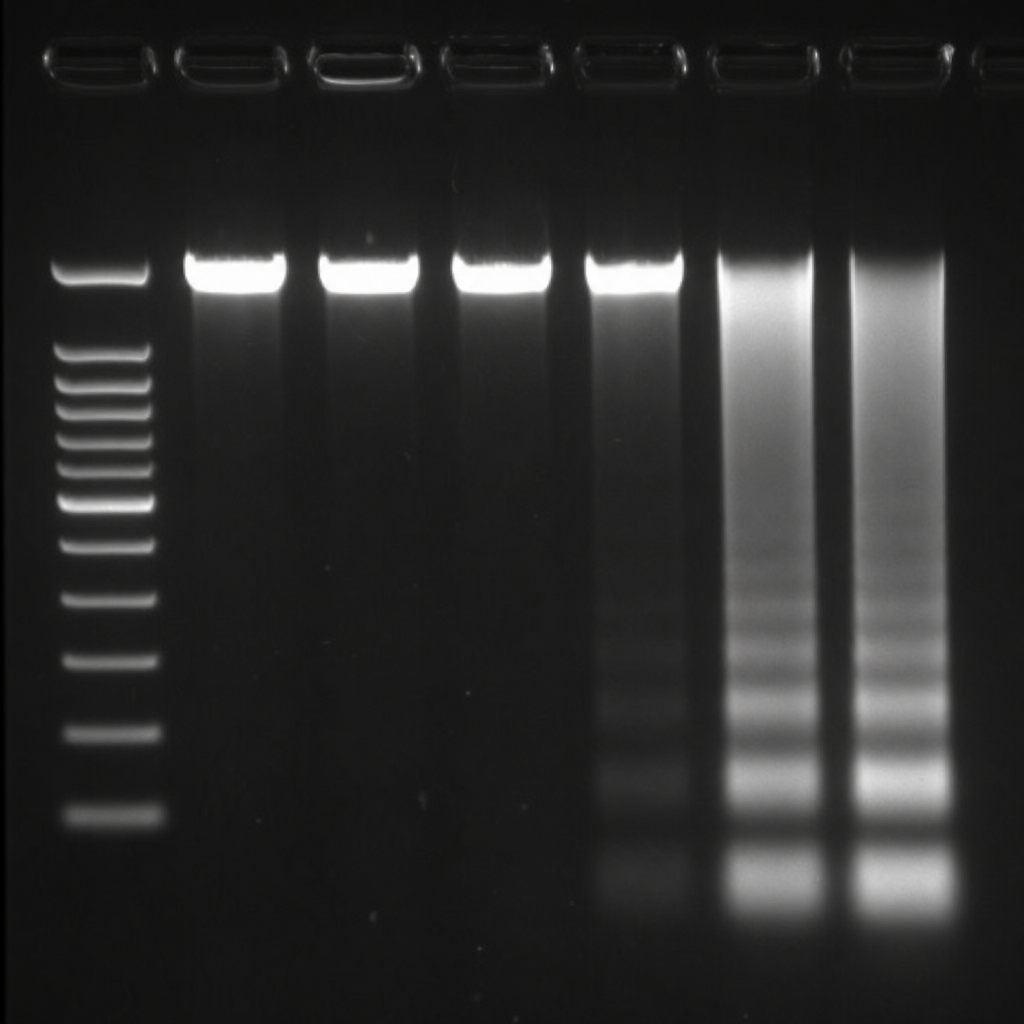
The given pattern of electrophoresis is obtained in which of the following conditions?
Hypercoagulability due to a defective Factor V gene is called?
Which of the following is an inhibitor of apoptosis?
What is the most common primary immunodeficiency?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app