
General Pathology — MCQs

On this page
Autosomal recessive disorders include all except :
Which one of the following is due to the monosomy of X-chromosome?
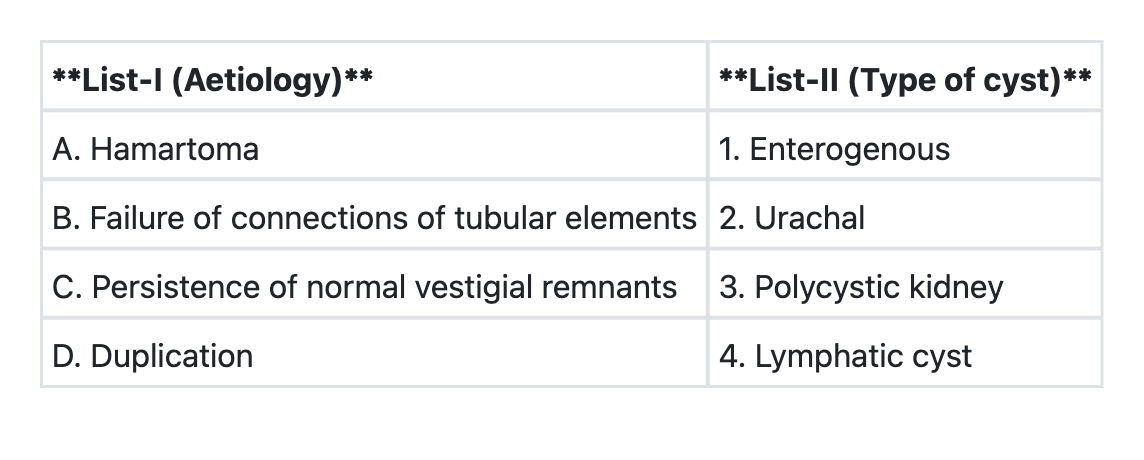
Match List-I with List-II and select the correct answer using the code given below the Lists:
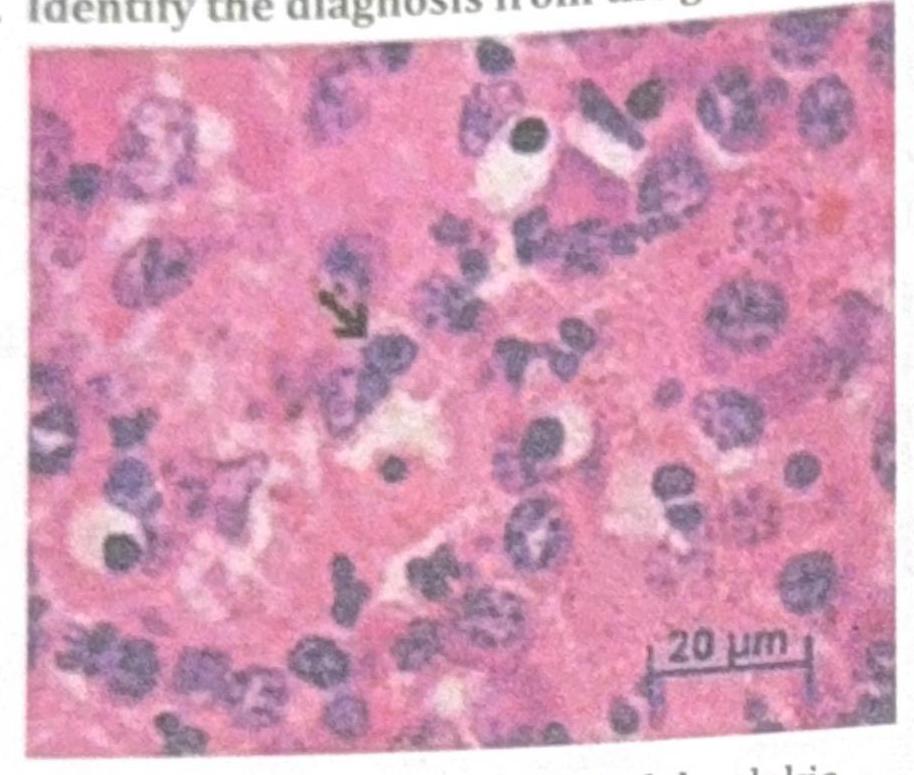
Identify the diagnosis from the given image
TTF-1 (Thyroid Transcription Factor-1) immunohistochemical marker is most commonly seen in which of the following?
A child undergoes prophylactic irradiation as preparation for bone marrow transplantation (BMT) for treatment of acute lymphoblastic leukemia (ALL). Which of the following cell types will be least affected by the radiation?
Iron in tissues is stained by:
A baby is being evaluated for delayed developmental milestones. On examination, the child has hepatosplenomegaly. A microscopic image of the bone marrow evaluation is shown below. What is the most appropriate treatment?

Abnormal accumulation of misfolded protein is seen in?
Order of drawing blood in vacutainers should be in the following sequence to prevent contamination?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app