
General Pathology — MCQs

On this page
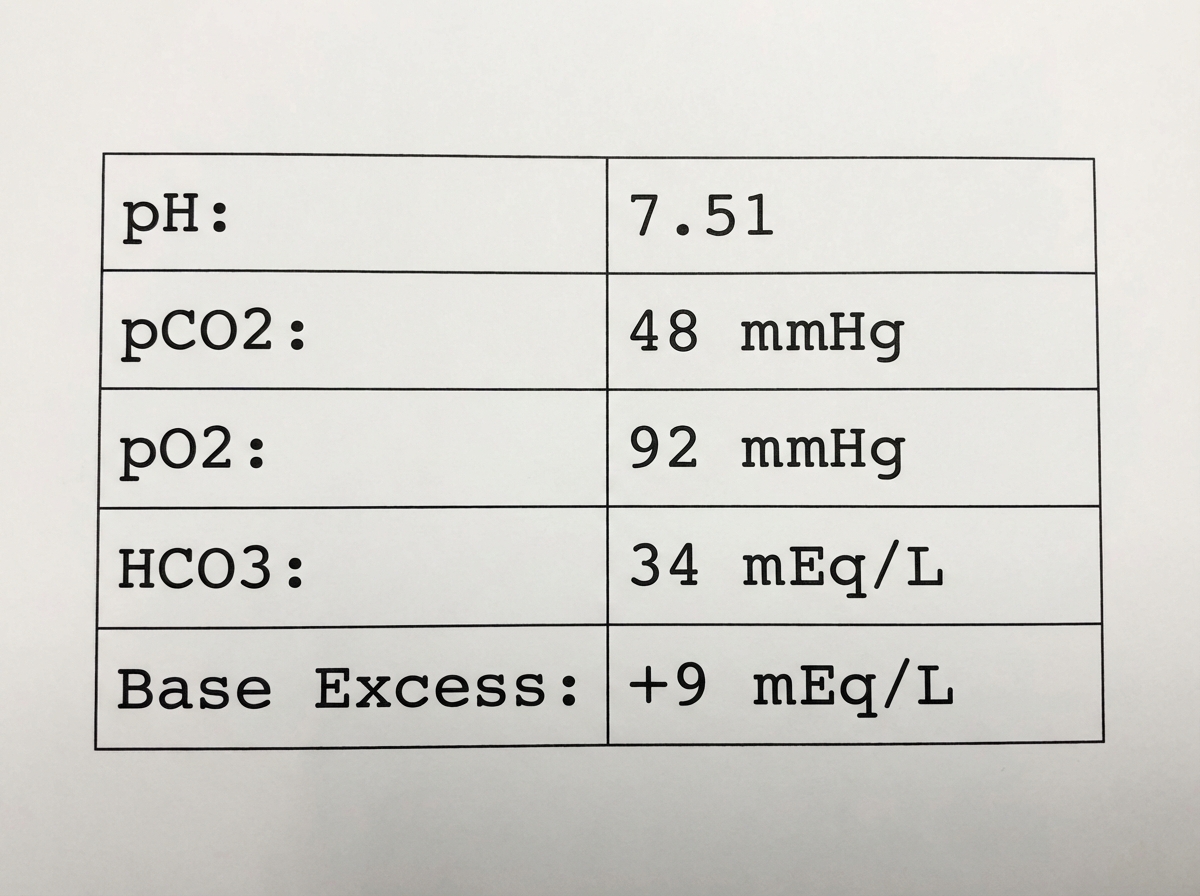
Which of the following disease processes best accounts for the arterial blood gas (ABG) abnormality shown in the image?
Autopsy of a specimen shows pale infarction. Pale infarct is seen in all of the following organs, EXCEPT:
The disease process that best accounts for this problem?

Autopsy of a specimen shows pale infarction. Pale infarct is seen in all of the following organs, EXCEPT:
Why do fetal cells continue to divide while terminally differentiated adult cells do not?
Which of the following cell types differentiates into a macrophage?
What term best describes nuclear dissolution?
All of the following are functions of CD4 helper cells, except?
A 40-year-old female patient complains of excessive bleeding and drowsiness following a road traffic accident 5 hours ago, with a lacerated wound on the lower back region. General physical examination reveals: Blood pressure - 80/60 mmHg, Jugular venous pressure - low, Pulsus paradoxus - present, Cardiac output - Increased. The patient is in which type of shock?
In amyloidosis of the tongue, where is the amyloid deposited primarily?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app