
General Pathology — MCQs

On this page
Multifactorial inheritance is seen in which of the following conditions?
Hepatolenticular degeneration is seen with the deposition of which metal?
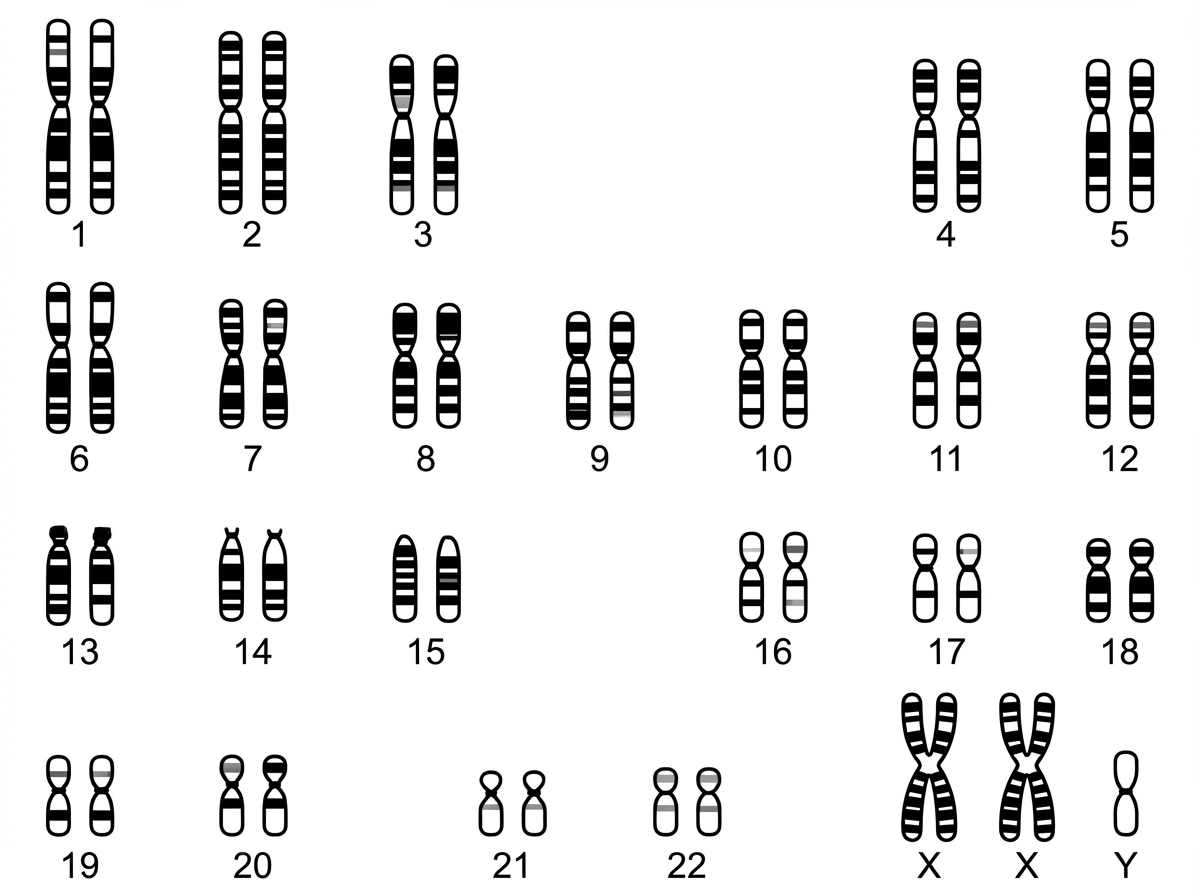
In the provided karyotype, which abnormality is observed? The karyotype shows 2 X-chromosomes and 1 Y-chromosome.
Metastatic calcification is most commonly seen in which of the following locations?
Metastatic calcification is most commonly seen in which of the following locations?
An overproduction of tissue normal to a particular area is called as what?
What is the inheritance pattern of the ABO blood group system?
Biopsy of the parotid gland in Sjogren's syndrome shows which of the following?
Ectopic ACTH production is most commonly seen in which of the following conditions?
HMB 45 is a tumor marker for which of the following conditions?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app