
General Pathology — MCQs

On this page
DNA integrity and replication are ensured at which stage of the cell cycle?
Which of the following is a characteristic of classical Mendelian inheritance of an autosomal dominant disease?
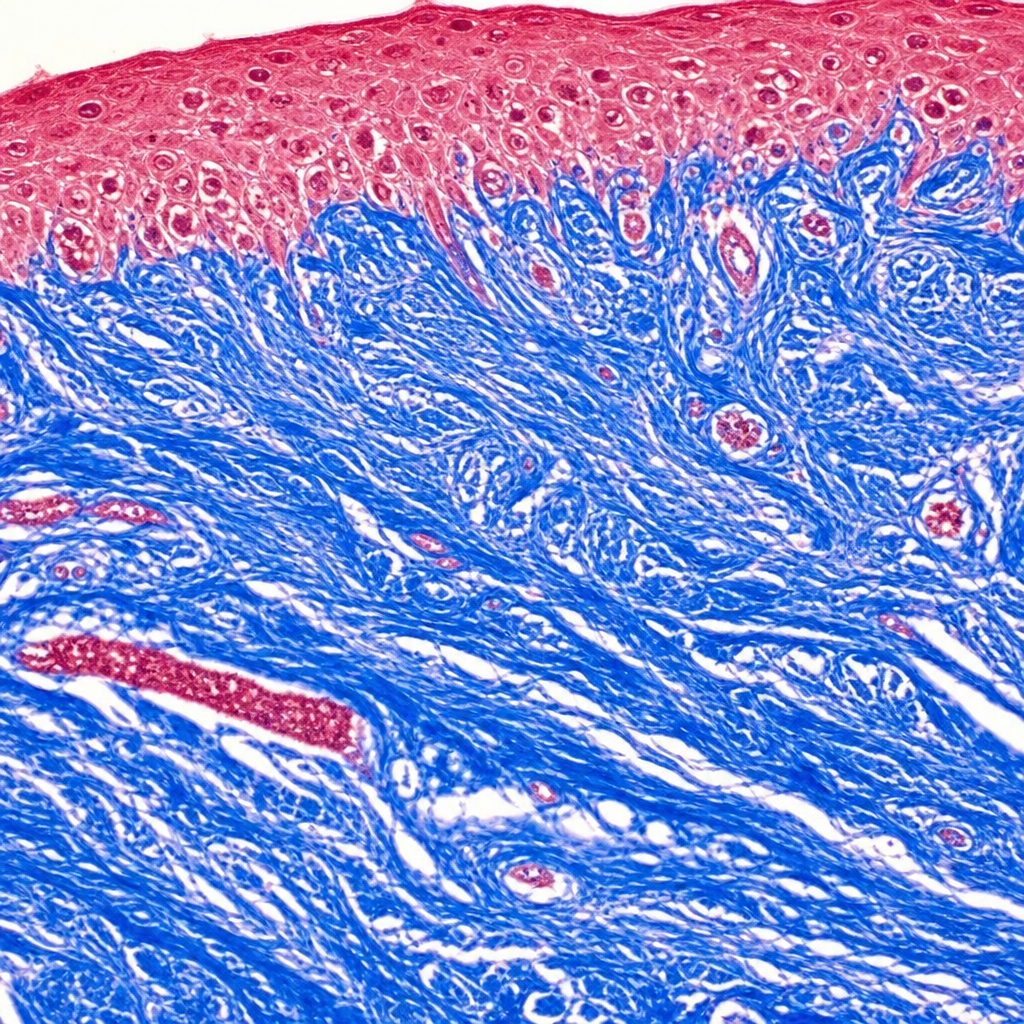
Which tissue component is highlighted blue by the shown Masson's trichrome stain?
Which of the following is true about metastatic calcification?
Crumpled tissue paper appearance of cytoplasm in bone marrow examination is due to the intracellular accumulation of which of the following?
Which of the following disorders is most commonly associated with Down's syndrome?
The type of embolism typically seen following fractures of long bones is:
A 40-year-old pregnant female in her third trimester presents with bilateral leg swelling. Which of the following statements about the type of thrombosis most likely to be present in this patient is true?
An increase in the size of a cell in response to stress is called hypertrophy. Which of the following does not represent an example of smooth muscle hypertrophy as an adaptive response to a relevant situation?
All of the following are features of stem cells except?
Practice by Chapter
Cell Injury and Cell Death
Practice Questions
Adaptations of Cellular Growth
Practice Questions
Accumulations and Deposits
Practice Questions
Acute and Chronic Inflammation
Practice Questions
Tissue Repair and Wound Healing
Practice Questions
Hemodynamic Disorders
Practice Questions
Genetic Disorders
Practice Questions
Environmental Pathology
Practice Questions
Nutritional Diseases
Practice Questions
Molecular Basis of Disease
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app