
Gastrointestinal Pathology — MCQs

On this page
Mark the correct statement regarding inflammatory bowel disease.
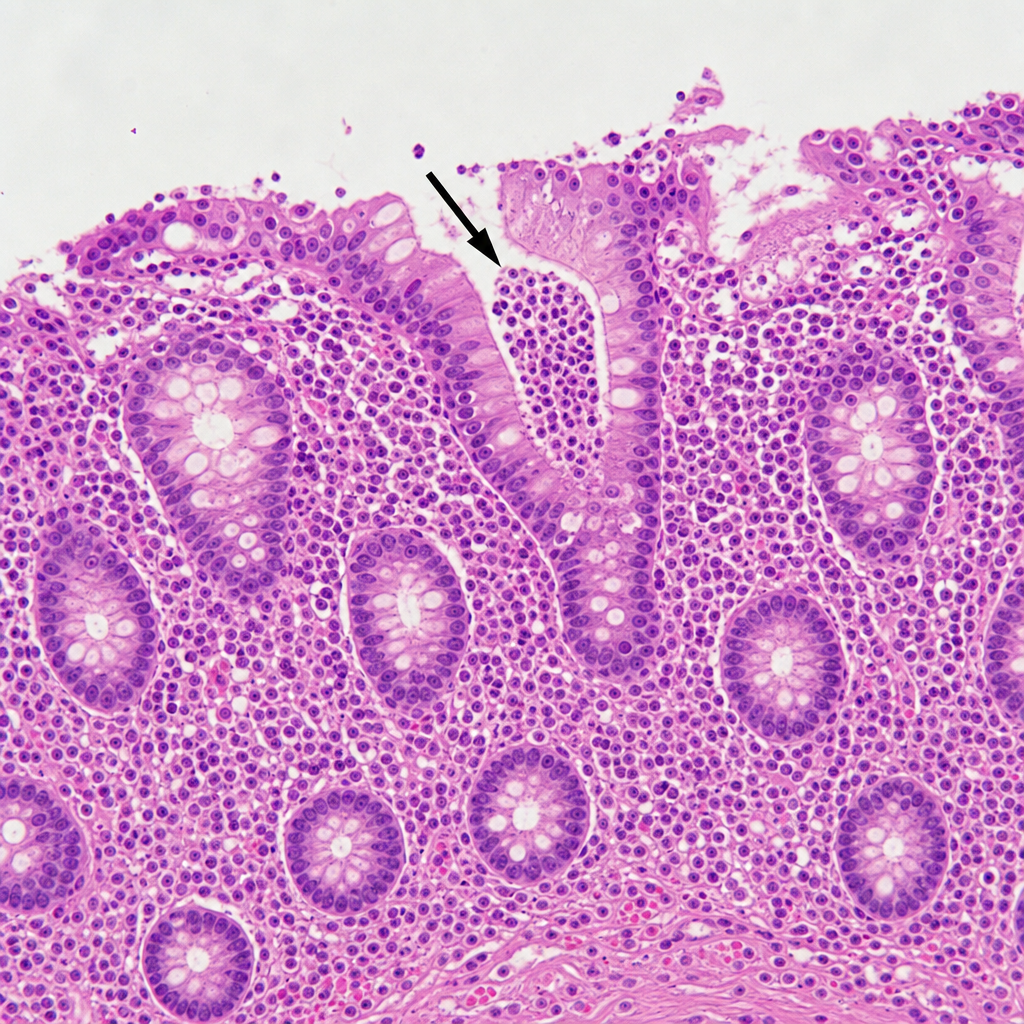
A 24-year-old man presents with recurrent abdominal pain, diarrhea with fatty porridge-like stools and occasional blood up to 8 times per day, joint pain, and weight loss. Ileocolonoscopy shows regions of erythema, swelling, and cobblestone-like appearance of the ascending colon and terminal ileum. Targeted biopsies are taken for evaluation. One of the slides, which underwent histological assessment, is shown in the image. Which of the following best describes the histologic finding marked with the black arrow?
All of the following special histology stains are used to demonstrate H. pylori in gastric biopsies, except:
Which of the following is true about carcinoid tumor?
Which among the following parotid tumors spreads through neural sheath
Hirschsprung disease has association with which of the following conditions?
Which of the following is not true regarding Whipple's Disease ?
Following is true about the incidence of tumors of salivary glands except -
Most common tumor of submandibular gland is -
Characteristic of amebiasis is:
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app