
Gastrointestinal Pathology — MCQs

On this page
The following specimen of esophagus and biopsy performed shows all except:
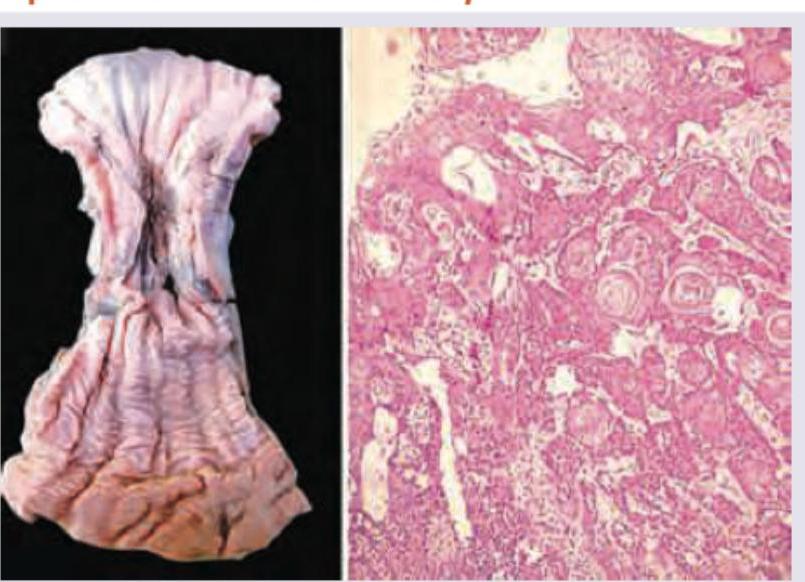
All are true about the condition shown except:
All are true about the esophageal condition shown in the image except:
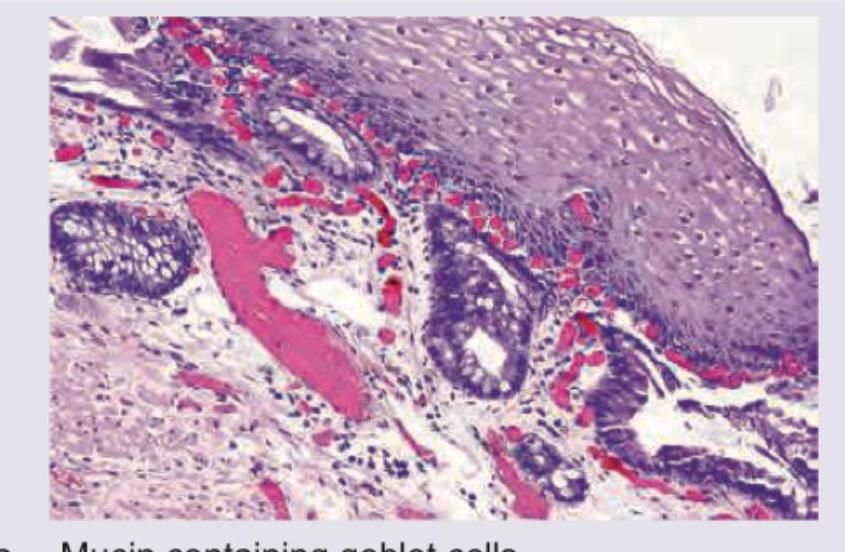
A 35-year-old male patient presents with a history of heartburn. An upper GI endoscopy was done and a biopsy from a suspicious lesion showed the following picture. What does this show? Which special stain will you use for confirmation and what will you look for?
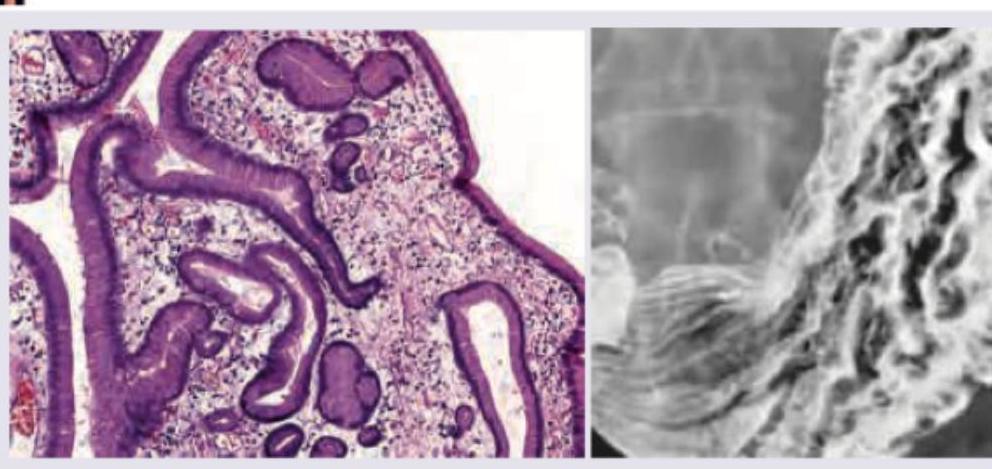
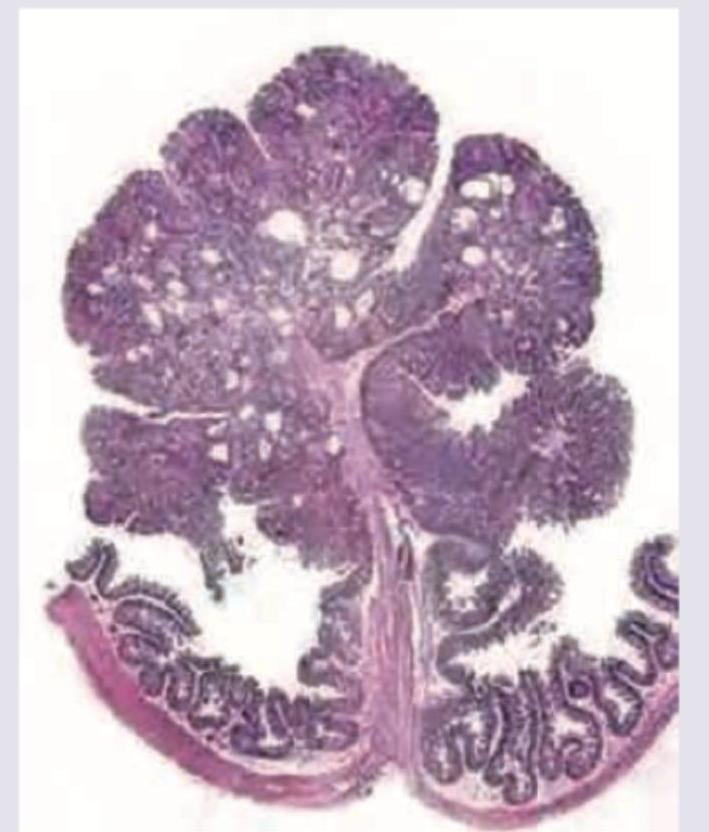
A 15-year-old patient develops intussusception for which he was operated and a segment of intestine showing multiple polyps was resected. The microscopy showed the following pathology. What is the likely diagnosis?
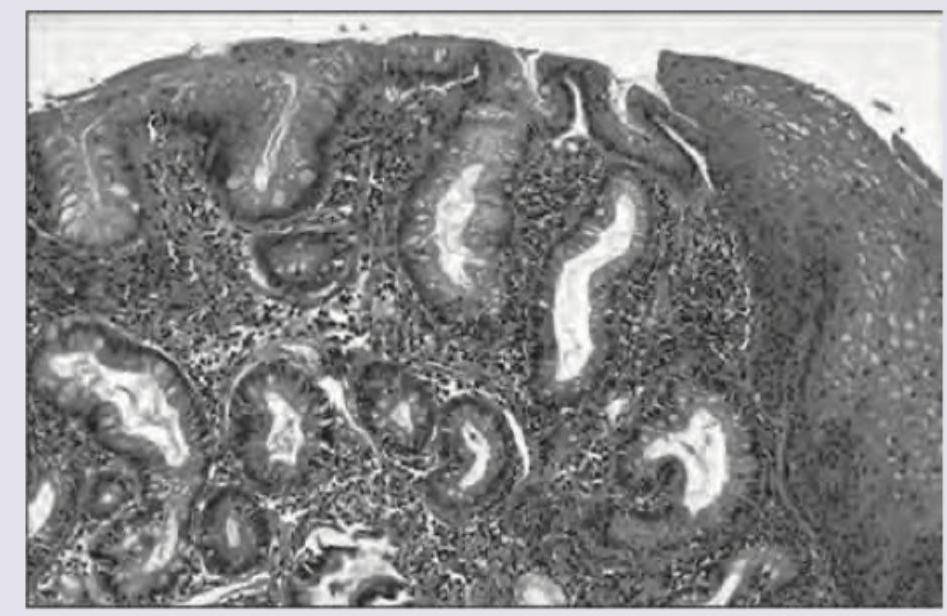
A 40-year-old patient presents with heart burn and increased salivation. UGI endoscopy was performed and biopsy was taken. What is the diagnosis? (AIIMS May 2017)

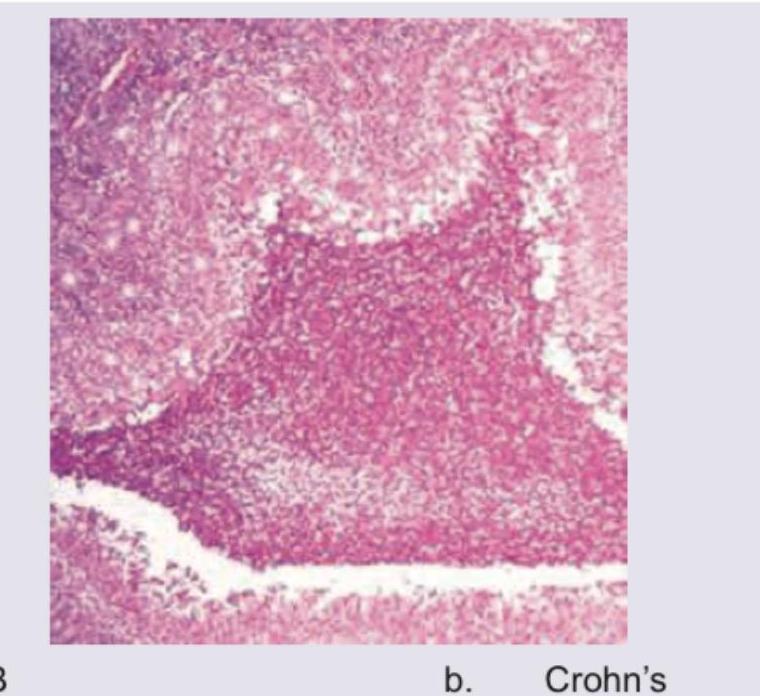
A 50-year-old male presents with colicky abdominal pain and recurrent bloody diarrhea. Colonoscopy shows geographical ulcers. Histopathology is shown below. Diagnosis is:
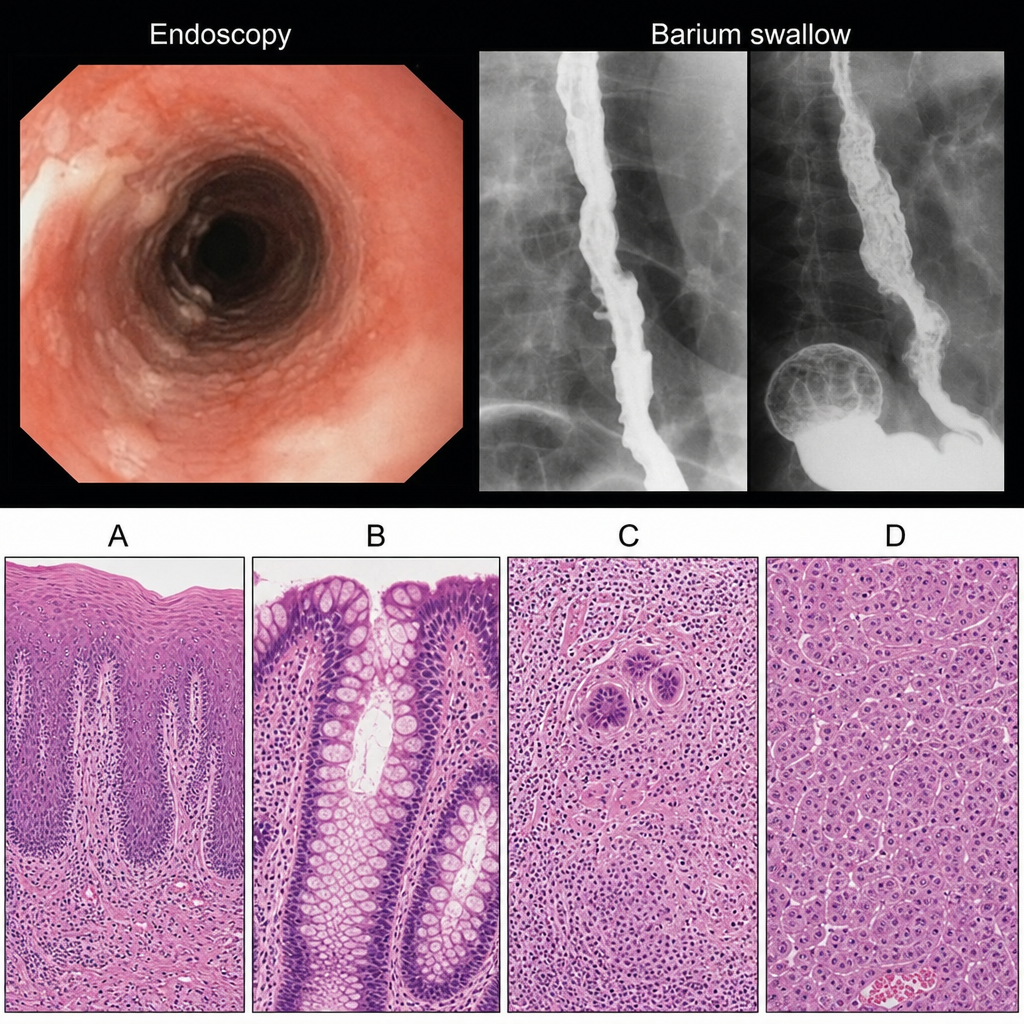
Endoscopic and Barium swallow findings of a patient are shown below. Select the correct histopathological slide of the patient.
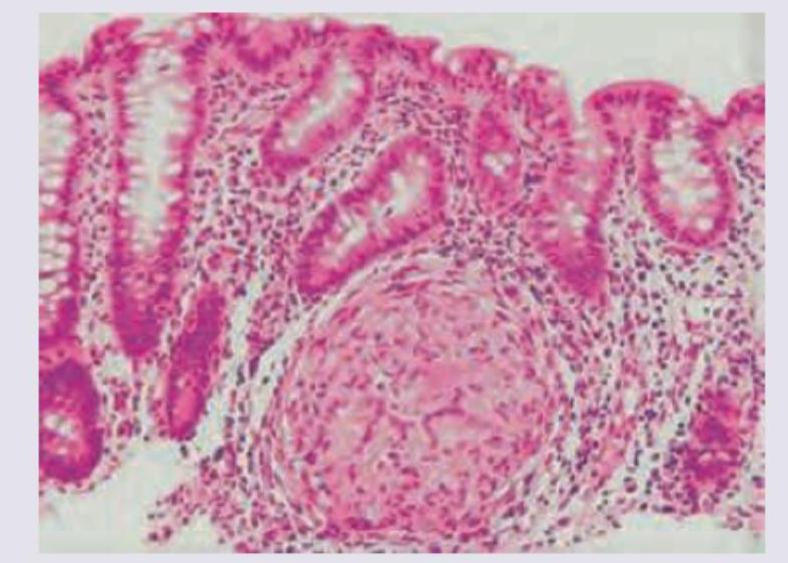
The image shows a histological section of intestinal tissue with a granuloma. What is the most likely diagnosis?
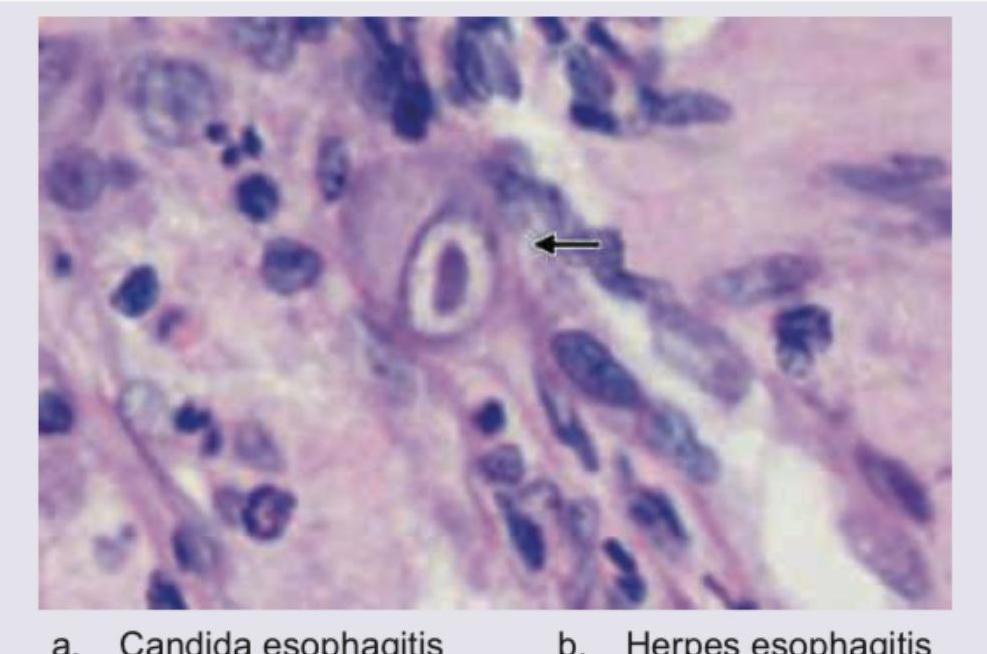
A 40-year-old immunocompromised patient presents with complaints of dysphagia. UGI endoscopy shows multiple ulcers in distal esophagus. Biopsy was performed and histopathology is shown below. Diagnosis is:
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app