
Gastrointestinal Pathology — MCQs

On this page
Why does not every Helicobacter pylori infection lead to ulcers?
Most common cause of squamous cell carcinoma at the base of the tongue is:
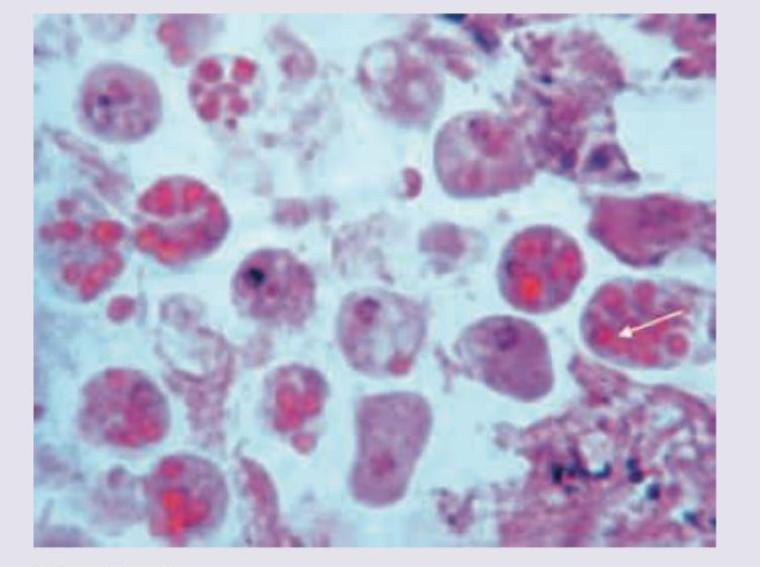
The following histological slide demonstrates:

A 23-year-old male presented with abdominal pain and bloody diarrhea of one week duration. The following colonoscopic biopsy is diagnostic of infection with:
A 32-year-old woman with a history of multiple hamartomas scattered throughout the small intestine presents to a physician for follow-up. All are true about her diagnosis except?
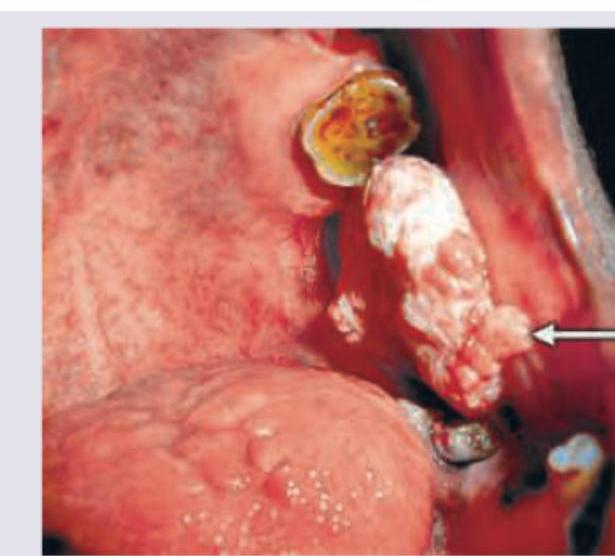
A 62-year-old male smoker and chronic alcohol user presents with a 3-month history of a rapidly growing, painful gingival lesion with bleeding. Examination reveals an indurated, irregular, ulceroproliferative mass on the alveolar margin with fixation to underlying bone. Biopsy confirms squamous cell carcinoma. What is the most likely diagnosis?
A 60-year-old man with long-term areca-nut/betel-quid or gutka chewing history presents with trismus and ankyloglossia. The lesion is shown below. Diagnosis is? (NEET Pattern 2018)

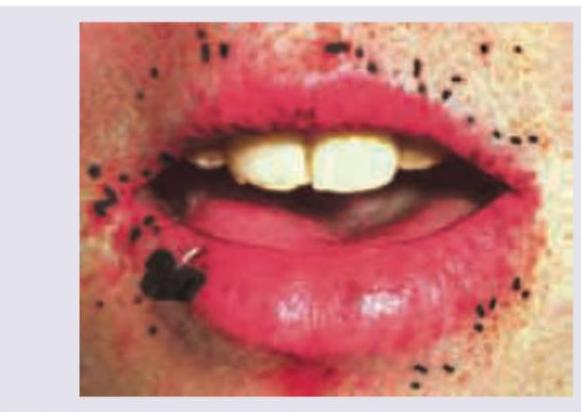
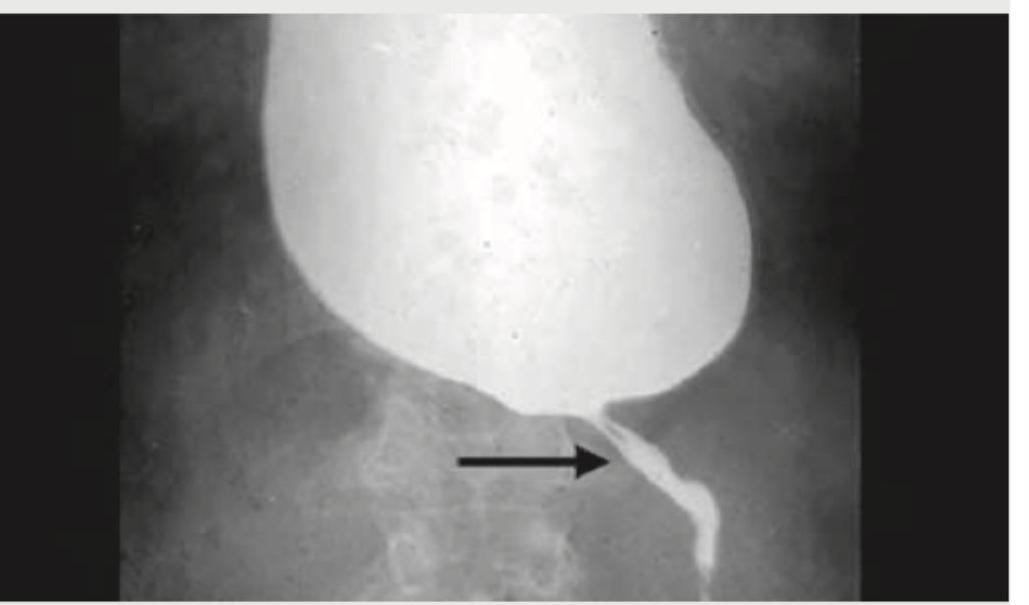
Which of the following is responsible for development of the disease, whose Barium swallow is shown below?
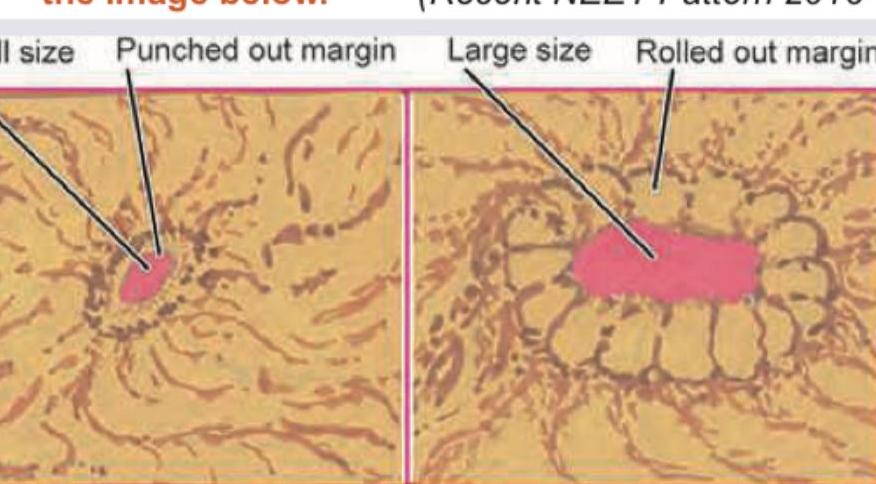
Identify the types of gastric ulcers labeled A and B in the image below.
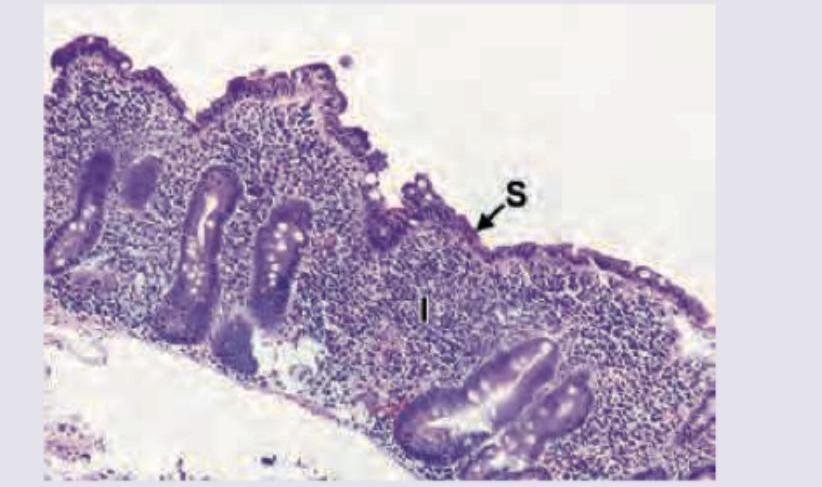
One-year-old child with failure to thrive and diarrhea. On examination anemia and puffy eyes are noted. Intestinal biopsy was performed. All are true about the condition shown except:
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app