
Gastrointestinal Pathology — MCQs

On this page
Helicobacter pylori causes all of the following except:
Acinic cell carcinomas of the salivary gland arise most often in which location?
Neoplastic transformation in leukoplakia is seen most commonly in which of the following locations?
What are the potential complications that can arise from a dentigerous cyst?
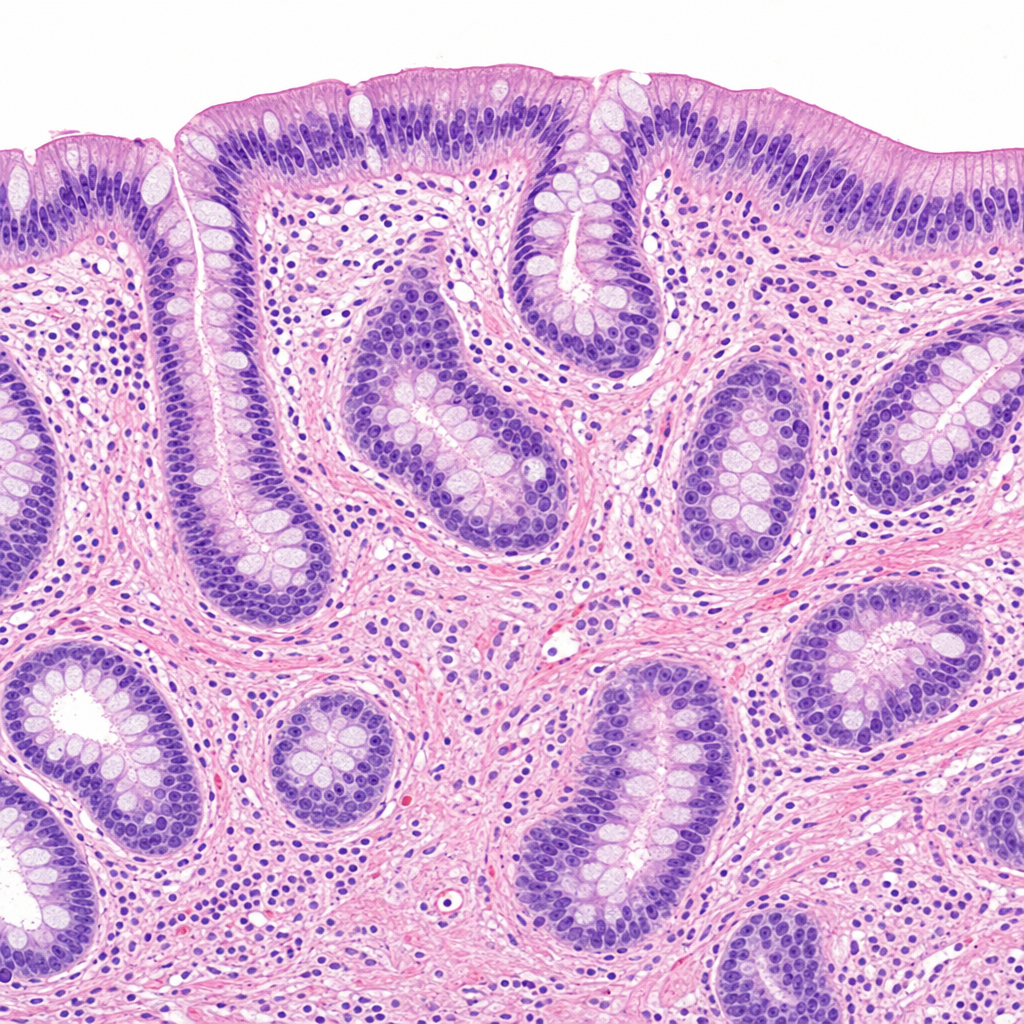
A 42-year-old man presents with long-standing abdominal pain after meals, relieved by antacids. He has lost 9 kg in the past year. Physical examination reveals peripheral edema and ascites. Laboratory studies show decreased serum albumin but normal serum levels of transaminases and gastrin. What pathologic changes would most likely be seen on examination of this patient's stomach?
All of the following are pre-malignant conditions except:
Which of the following is FALSE about hypertrophic gastropathy?
Sloughing of necrotic epithelium is characteristic of:
A 60-year-old male with a long history of chronic gastroesophageal reflux disease (GERD) presented with dysphagia. A mucosal biopsy from the distal esophagus was performed, as shown in the image. What is the most likely finding on histology?
Helicobacter pylori has been implicated in all of the following conditions except:
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app