
Gastrointestinal Pathology — MCQs

On this page
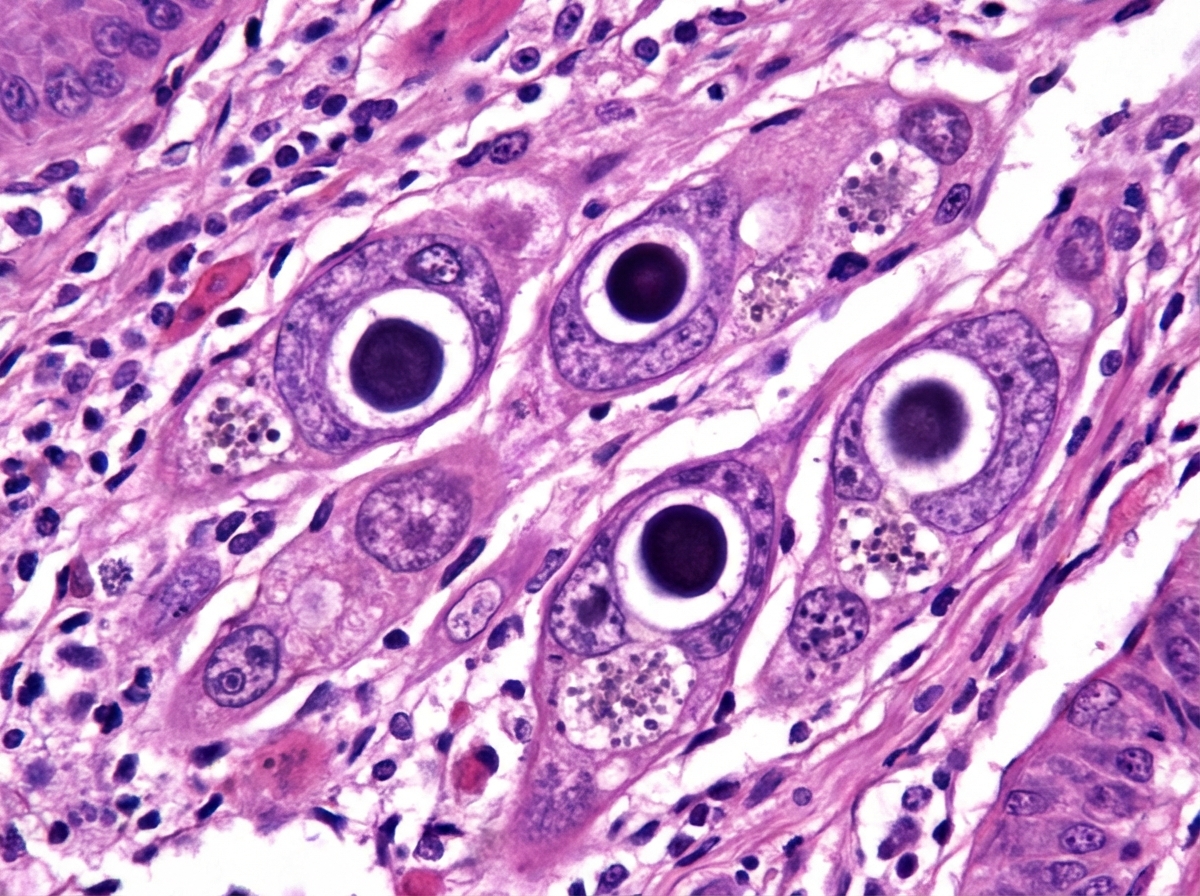
A 45-year-old HIV-positive male presented with dysphagia. Endoscopy and biopsy were performed. What is the most likely diagnosis based on the endoscopic and histological findings?
Which of the following is NOT a gene involved in the pathogenesis of gastric cancer?
A patient with intestinal malabsorption shows marked improvement when flour products are removed from the diet. At the height of the disease, what histologic changes would be seen at which of the following sites?
Malignant gastric ulcers are characterized by which of the following?
Which of the following is NOT a pathologic feature of H. pylori chronic gastritis?
Which statement is false regarding familial adenomatous polyposis?
A 45-year-old woman presents with increasing abdominal girth over the past 2 years. Physical examination reveals abdominal distension. A CT scan shows multiple nodules on peritoneal surfaces along with low-attenuation mucinous ascites. Cytological examination after paracentesis showed well-differentiated columnar cells with minimal nuclear atypia. From which site did this pathology most likely originate?
Which of the following conditions is NOT typically associated with the formation of a small intestinal stricture?
Turcot's syndrome is associated with which of the following conditions?
A segment of jejunum shows a nodular lesion in the submucosa. Histological examination reveals a tumor composed of uniform round cells arranged in trabeculae, with a "salt-and-pepper" chromatin pattern. Electron microscopy shows secretory granules, and immunohistochemistry is positive for serotonin. Which of the following parameters best correlates with the metastatic potential of this tumor?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app