
Gastrointestinal Pathology — MCQs

On this page
Entero-enteric fistula is found in all EXCEPT:
What is the pathogenesis of a periapical cyst?
Low dietary fiber intake is related to which carcinoma?
Which of the following is FALSE regarding autoimmune atrophic gastritis?
A 45-year-old businesswoman arrives with vague abdominal complaints and has noticed melenic stool. A sigmoidoscopy reveals a 4-cm mass in the upper colon. Which tumor marker should be ordered?
Duke's stage C2 refers to carcinoma:
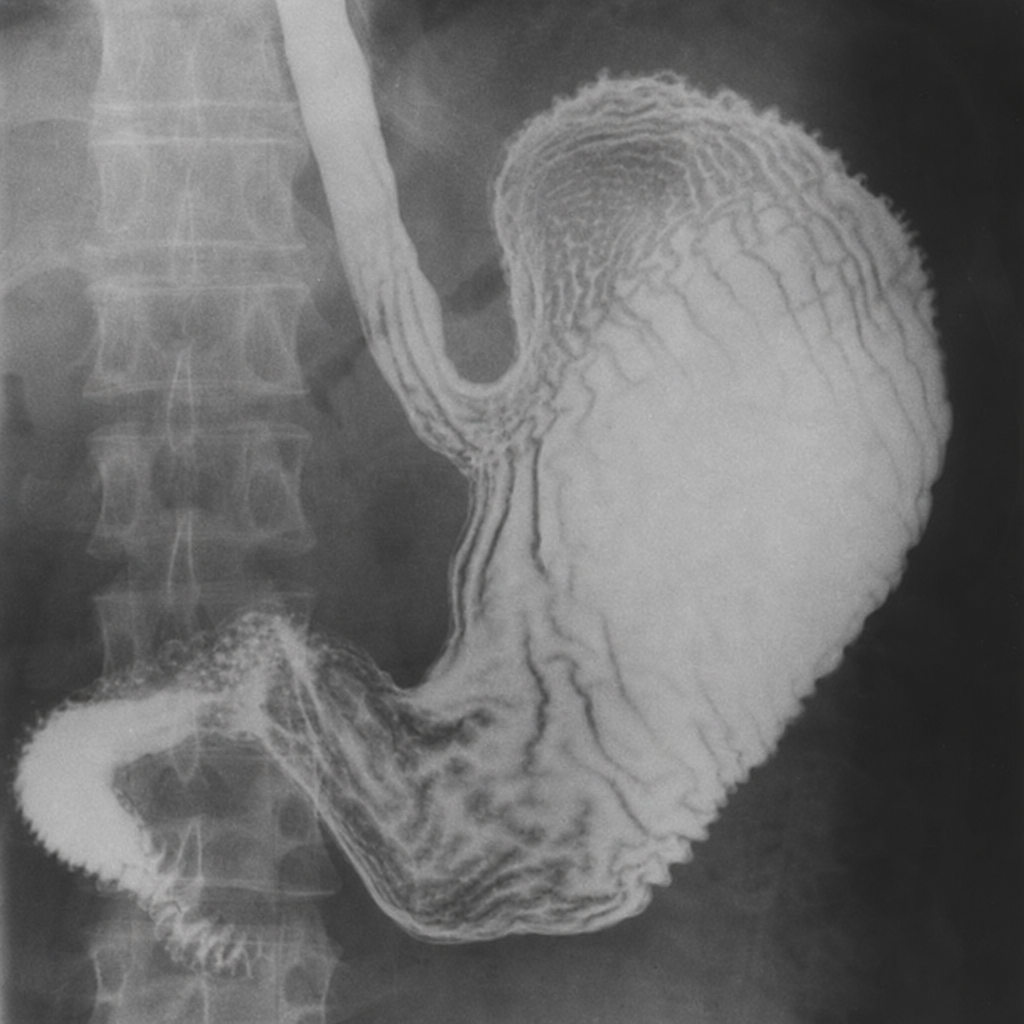
What is the diagnosis?

What is the diagnosis?
Which of the following is NOT considered a premalignant condition?
A peptic ulcer is associated with all of the following conditions except one?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app