
Gastrointestinal Pathology — MCQs

On this page
Which of the following colonic pathologies is thought to have no malignant potential?
Transmural inflammation with skip lesions in the colon are characteristic of which condition?
What is the most common type of cancer affecting the anus?
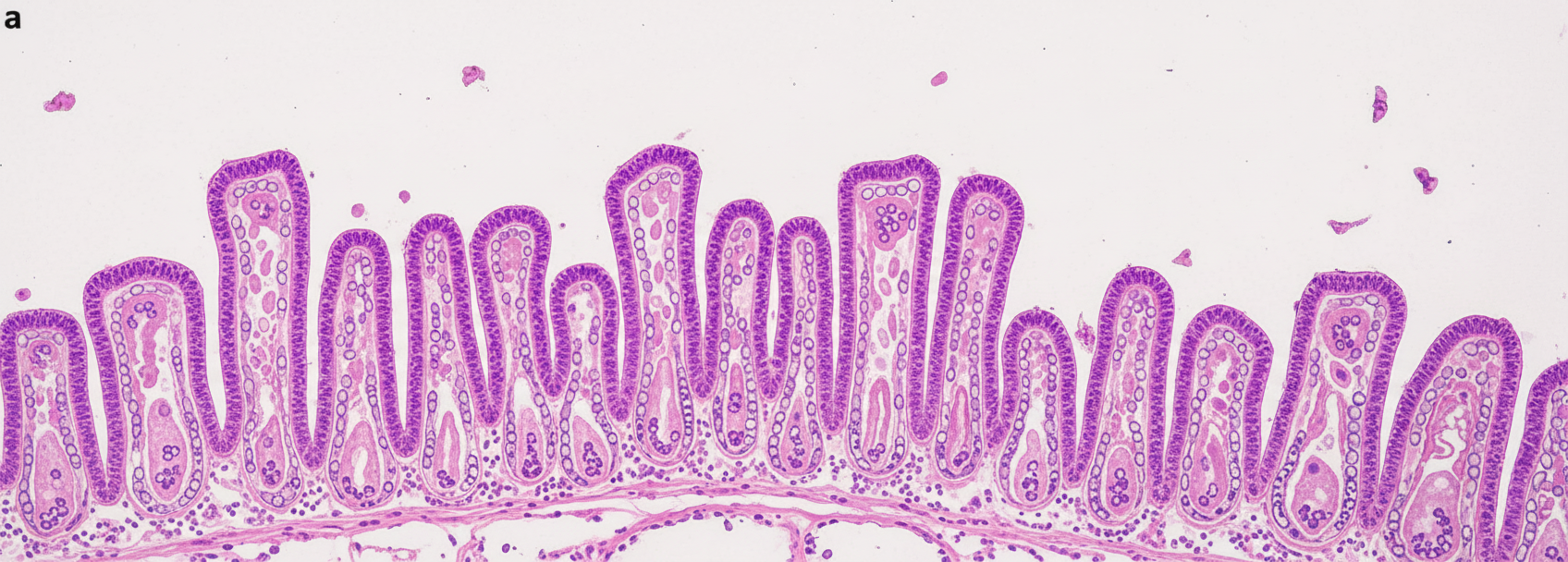
Diarrhea with acanthocytosis is seen in which of the following conditions?
A 40-year-old tobacco chewer undergoes a routine oral examination. Non-scrapable white patches are noticed on the left buccal mucosa. What histological examination findings are expected?
A 25-year-old male presents with a history of chronic diarrhea. Pathological examination reveals cryptitis and crypt abscesses. What is the likely diagnosis?
A 61-year-old man presents with 5 months of increasing fatigue, early satiety, and nausea, and vomited dark granular material yesterday. Endoscopy reveals a large ulcerated mass in the gastric fundus. Biopsies show a mass composed of spindle cells positive for c-Kit by immunohistochemistry with frequent mitoses. A 10-cm circumscribed mass is resected from the gastric wall. Which of the following therapies is most likely to be a useful adjunct in the treatment of his disease?
Which of the following conditions is characterized by a cobblestone appearance of the oral mucosa?
Which of the following statements about Familial Polyposis Coli is false?
A 60-year-old male presents with dysphagia. A distal esophageal mucosal biopsy is provided. What does it show?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app