
Gastrointestinal Pathology — MCQs

On this page
In which one of the following salivary gland tumors, the tumor is composed of "intermediate cells" histologically?
Which of the following is NOT true about solitary rectal ulcer syndrome?
Tobacco usage has been associated with which of the following oral pathological changes?
A 63-year-old man undergoes a screening colonoscopy and is found to have a polyp in his sigmoid colon. Which type of polyp is most associated with malignancy?
Zollinger-Ellison syndrome is not caused by tumors from which of the following organs?
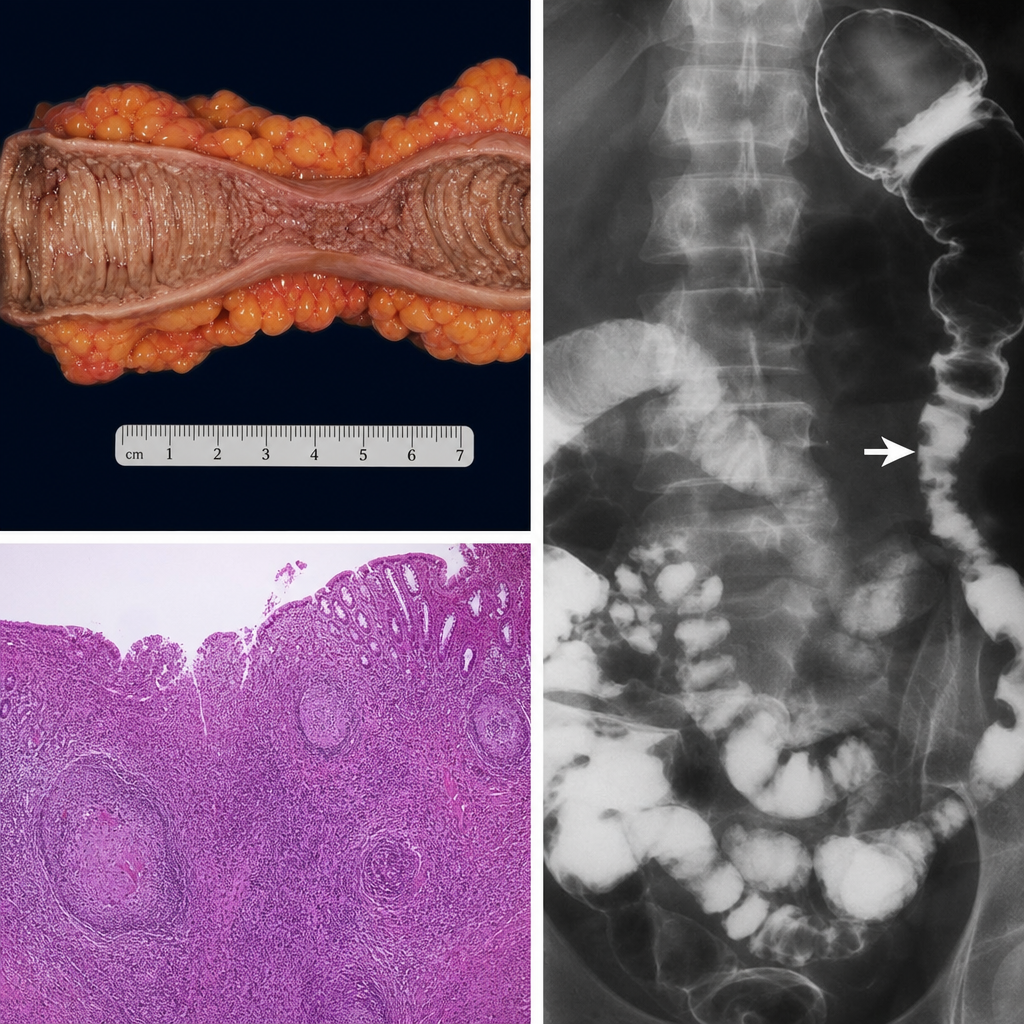
Which of the following conditions is most likely depicted in the image?
In which of the following conditions is acquired (secondary) megacolon seen?
All are true regarding foregut carcinoid tumors, except?
Stress-induced ulcers are most commonly found in which part of the gastrointestinal tract?
Helicobacter pylori is known to cause all of the following except?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app