
Gastrointestinal Pathology — MCQs

On this page
All of the following are true about Barrett's esophagus, EXCEPT:
A 58-year-old woman undergoes routine colonoscopy. A 2-cm submucosal nodule is identified in the appendix. Biopsy of the nodule shows nests of cells with round, uniform nuclei. Electron microscopy reveals numerous neuroendocrine granules in the cytoplasm. This patient's neoplastic disease is associated with which of the following clinical features?
A salivary gland tumor that histologically shows a double layer of epithelial cells based on a reactive lymphoid stroma is:
A 71-year-old male presents with dysphagia and is found to have a 5-cm mass that is located in the middle third of the esophagus and extends into adjacent lung tissue. A biopsy from this mass would most likely reveal?
The presence of anti-Saccharomyces cerevisiae antibody is a surrogate marker of which of the following conditions?
All of the following genes are implicated in colon carcinoma by the classical pathway except?
Gardner's syndrome is a rare hereditary disorder involving the colon. It is characterized by
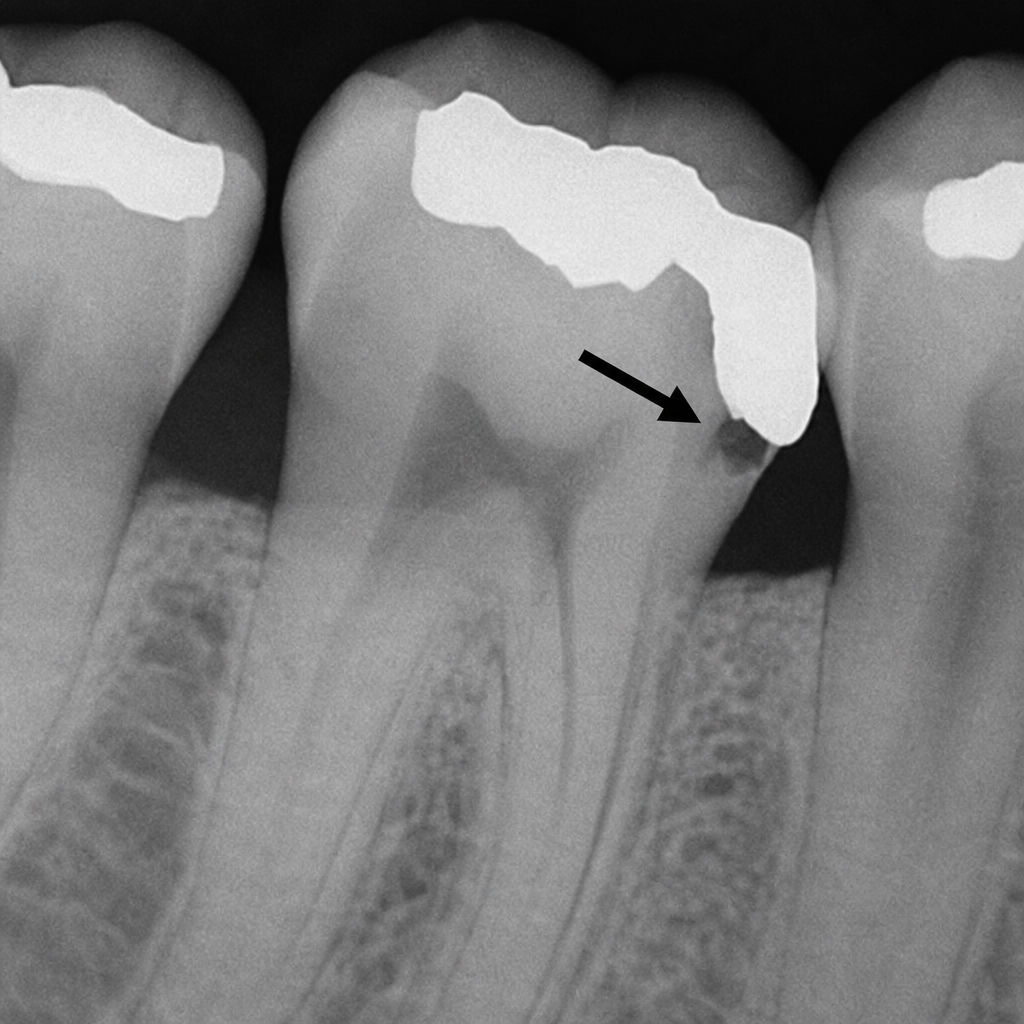
The carious lesion marked by the arrow represents:
All of the following are true about pleomorphic adenoma EXCEPT:
Pseudopolyposis is seen in which of the following conditions?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app