
Gastrointestinal Pathology — MCQs

On this page
Increased incidence of carcinoma is observed with which of the following conditions?
Hirschsprung disease is characterized by which of the following pathological findings?
In ulcerative colitis, colorectal cancer arises from which of the following?
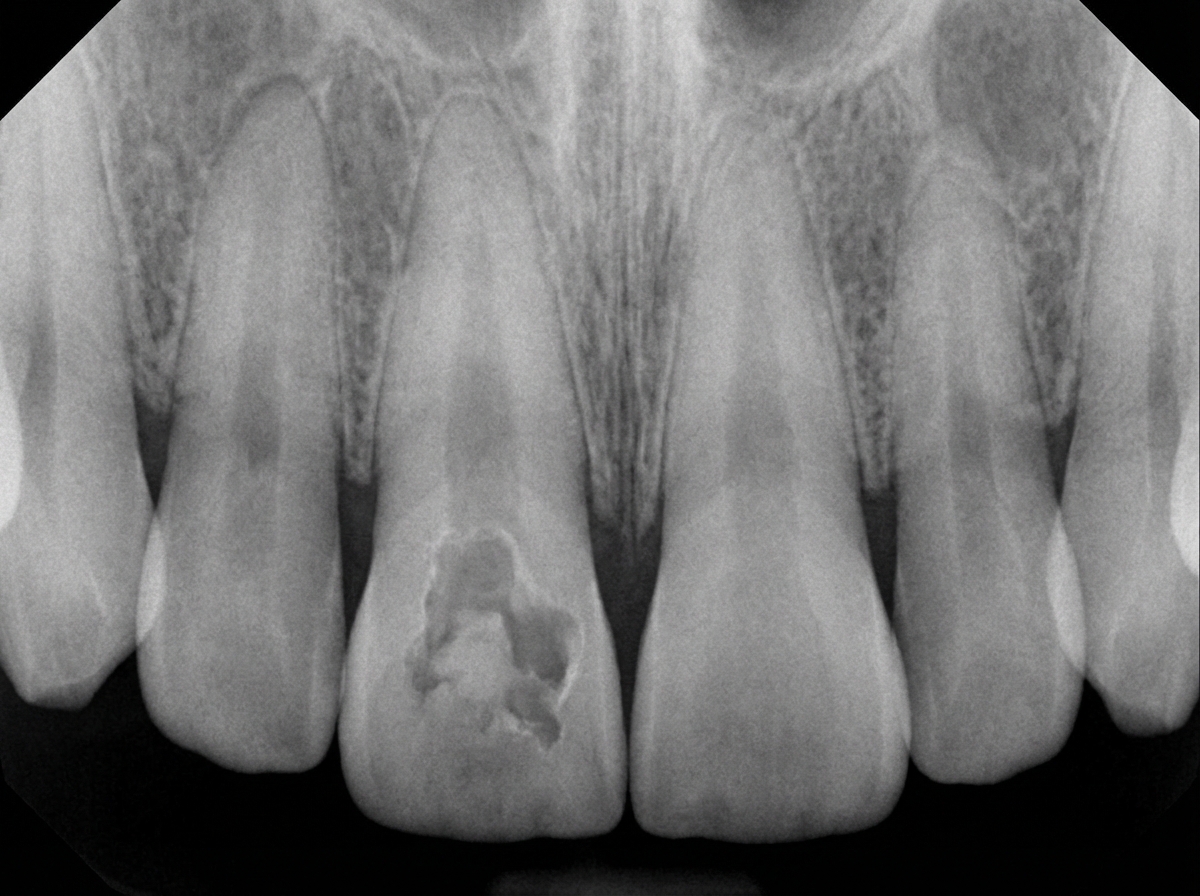
A patient gives a history of previous chronic abscess on the deciduous precursor of tooth 11. The following radiograph indicates:
Carcinoma of the colon develops in all patients with:
Which dietary factor is most strongly associated with colon carcinoma?
What is the pattern of inheritance for Gardner syndrome?
What is the most common primary malignant neoplasm of the small bowel?
Cobblestone appearance is seen in which of the following conditions?
E-cadherin mutation is seen in which type of gastric carcinoma classification?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app