
Gastrointestinal Pathology — MCQs

On this page
What structure arises from the apex of an infected non-vital tooth?
Which proto-oncogene is involved in Gastrointestinal Stromal Tumors (GIST)?
A patient presents with diarrhea, malabsorption, abdominal pain, and arthralgia. Intestinal biopsy reveals PAS-positive organisms within macrophages. What is the most likely diagnosis?
A 50-year-old male presents with a history of Gastroesophageal reflux disease. What is the most common pathological finding associated with this condition?
What is the most common type of gastric polyp?
What is the most important prognostic indicator in esophageal carcinoma?
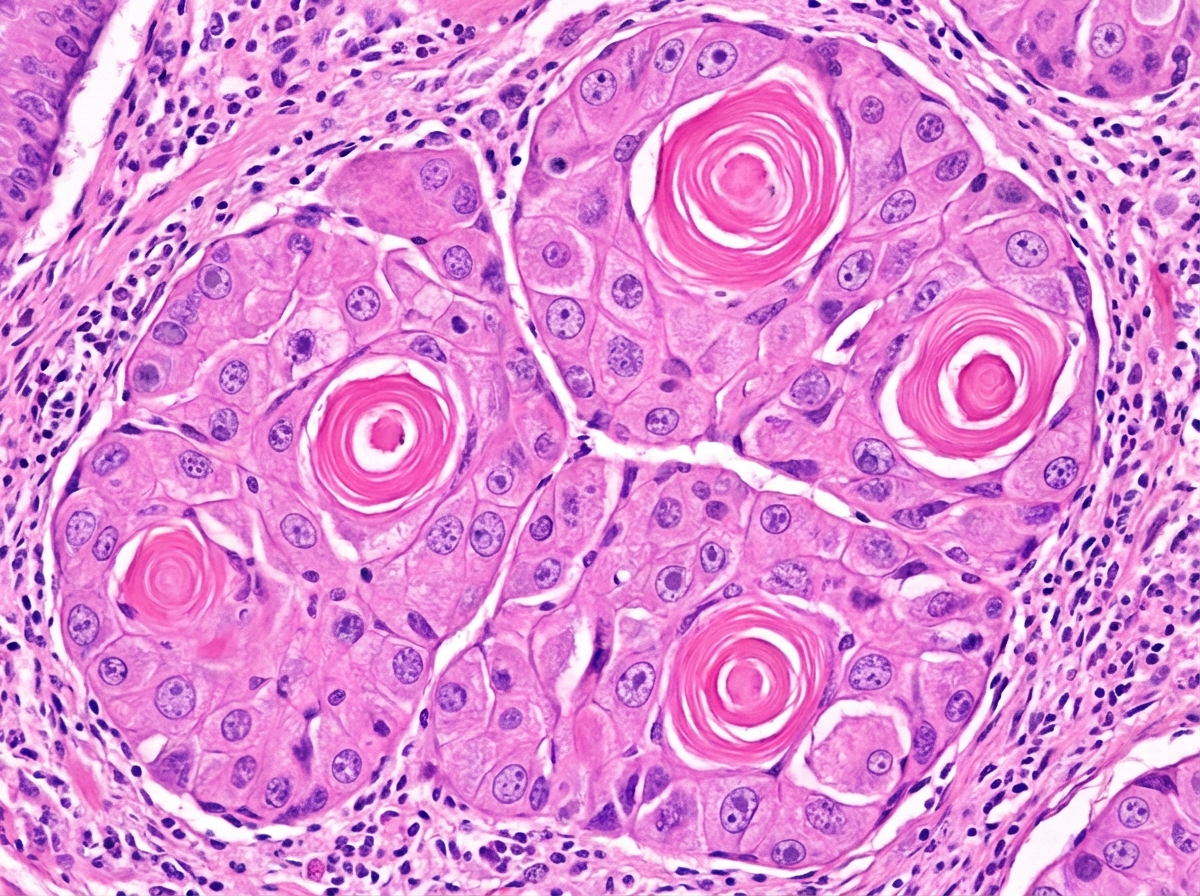
A 60-year-old patient with a prolonged history of tobacco chewing presents with symptoms of weight loss and dysphagia. An esophageal biopsy from an exophytic mass is shown below. What is your likely diagnosis?
Which of the following is an important risk factor for the development of squamous cell carcinoma?
Which of the following anaemias is a risk factor for the development of gastric carcinoma?
Type B gastritis is characterized by predominance in which region of the stomach?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app