
Gastrointestinal Pathology — MCQs

On this page
Which of the following statements concerning carcinoma of the esophagus is true?
Adenocarcinoma in the esophagus most commonly occurs in association with which of the following conditions?
Anal cancer is associated with which of the following viruses?
A patient presents with symmetrical, persistent, and painless swelling of the lacrimal and salivary glands. The patient reports no or minimal xerostomia and shows a positive response to steroid therapy. What is the most likely diagnosis?
Hourglass deformity is seen in which of the following conditions?
Which of the following is NOT true regarding Barrett's esophagus?
A patient has an increased number of columnar cells in the lower esophagus. Which of the following histological changes is present?
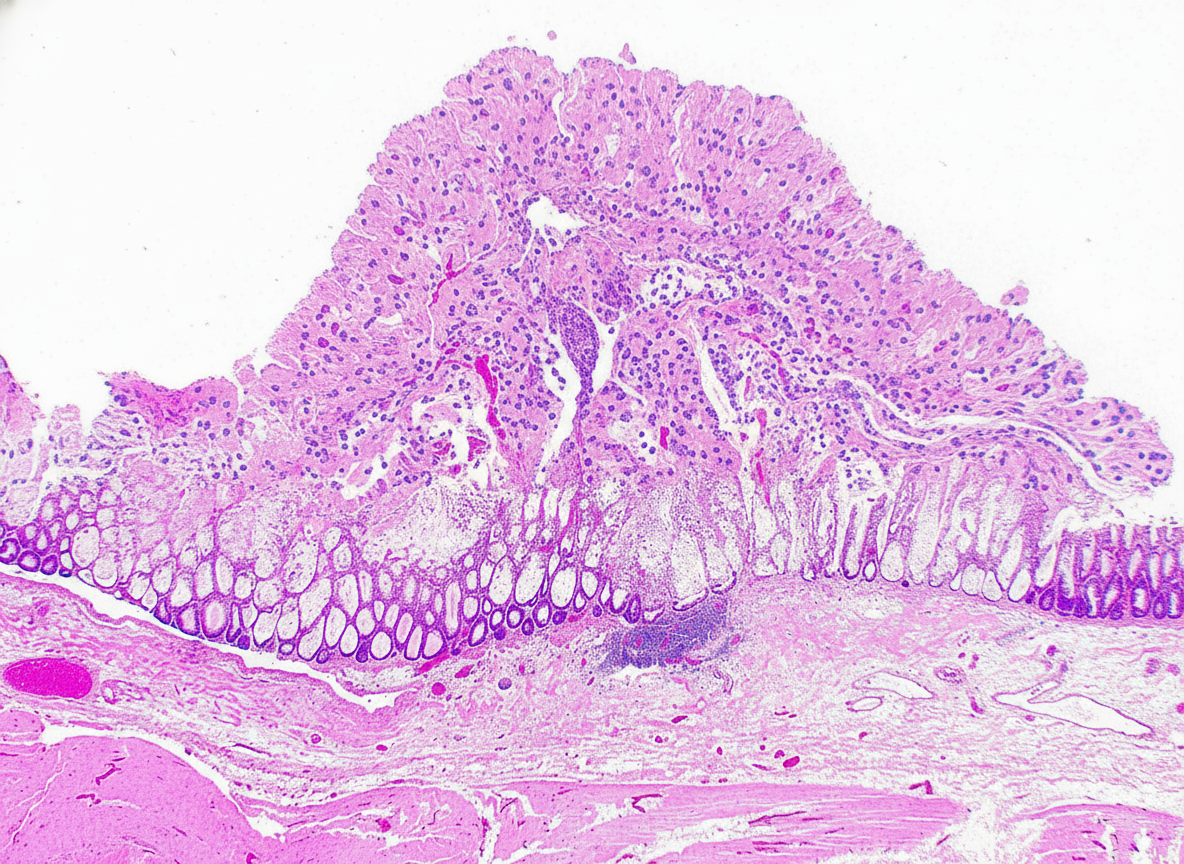
An elderly male with a history of long-term antibiotic intake presents with profuse watery diarrhea and abdominal cramps. The colonoscopic biopsy findings are shown in the image. What is the most likely diagnosis?
Which condition involves the entire thickness of the bowel wall with skin lesions?
What is the most common extra-intestinal malignancy associated with Hereditary Non-Polyposis Colorectal Cancer (HNPCC)?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app