
Gastrointestinal Pathology — MCQs

On this page
Multiple strictures in the intestine are found in which of the following conditions?
A 5-year-old boy presents with a one-week history of diarrhea, characterized by an average of six low-volume stools per day that are mucoid and sometimes blood-tinged. Physical examination reveals a temperature of 37.4°C, mild lower abdominal tenderness, and no palpable masses. Stool culture is positive for Shigella sonnei. Which of the following microscopic findings would most likely be observed in the colon of this child?
A 65-year-old woman has noticed a slowly enlarging nodule on her face for the past 3 years. On physical examination, a 3-cm, nontender, mobile, discrete mass is palpable on the left side of the face, anterior to the ear and just superior to the mandible. The mass is completely excised, and histologic examination shows ductal epithelial cells in a myxoid stroma containing islands of chondroid like tissue and bone. This patient is most likely to have which of the following neoplasms?
Absence of myenteric ganglion is seen in which condition?
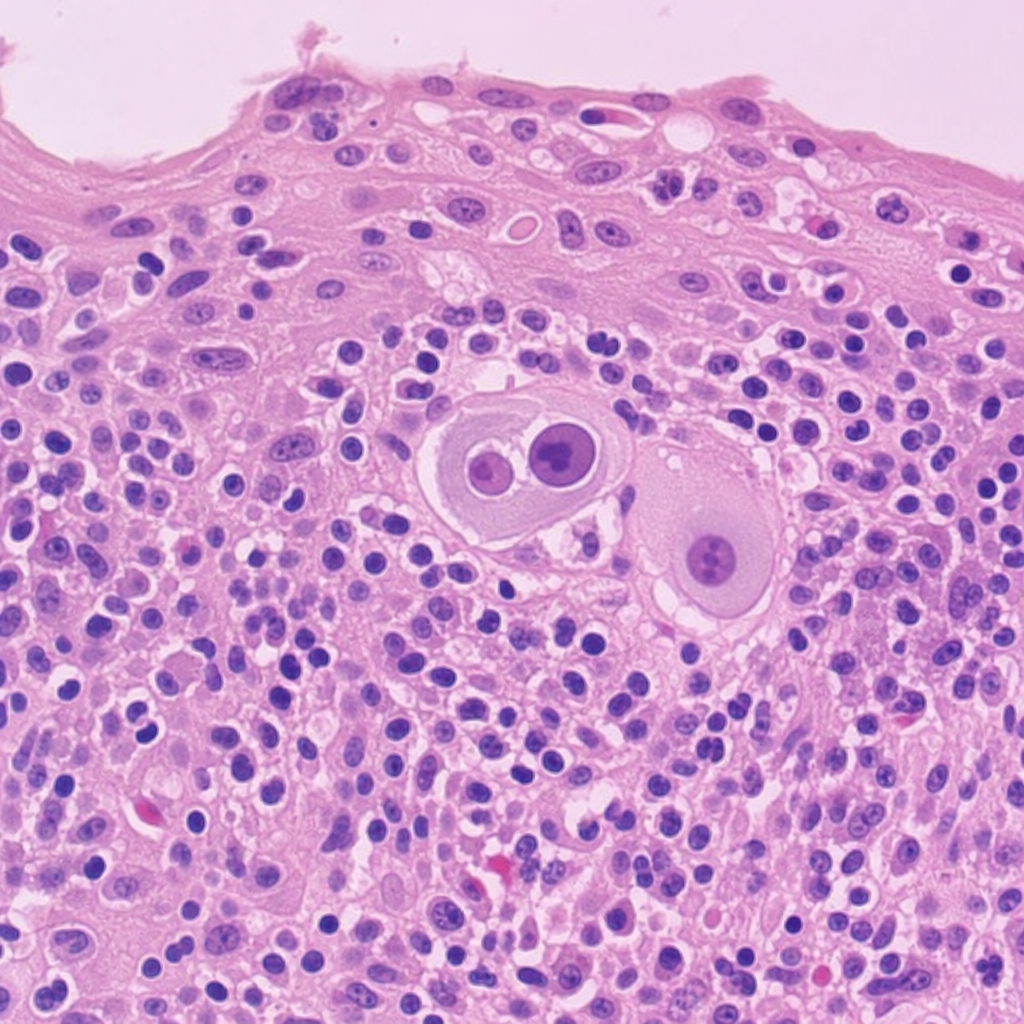
A 40-year-old immunocompromised patient presents with dysphagia. Upper GI endoscopy reveals multiple ulcers in the distal esophagus. Biopsy from the esophagus shows characteristic findings. What is the most likely diagnosis?
Which of the following is a precancerous condition of the stomach?
Which of the following is true regarding Crohn's disease?
Which of the following is NOT a characteristic of ulcerative colitis progressing to malignancy?
A biopsy of a small, rounded rectal polyp demonstrates glands and saw tooth crypts composed of a proliferation of goblet and columnar epithelial cells. No atypia is seen. This polyp is best classified as which of the following?
A 40-year-old immunocompromised patient presented with complaints of dysphagia. Upper GI endoscopy showed multiple serpiginous ulcers in the distal esophagus. Biopsy from the esophagus showed characteristic findings. What is the diagnosis?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app