
Gastrointestinal Pathology — MCQs

On this page
Which of the following gastric polyps does not undergo malignant transformation?
All of the following statements about carcinoid syndrome are true EXCEPT?
What is the most common site for lymphoma in the gastrointestinal tract?
Which of the following is NOT associated with Helicobacter pylori infection?
All of the following statements are true for telangiectasia of the colon EXCEPT:
Macrophages containing PAS-positive granules and rod-shaped bacilli are found in which condition affecting the small intestinal mucosa?
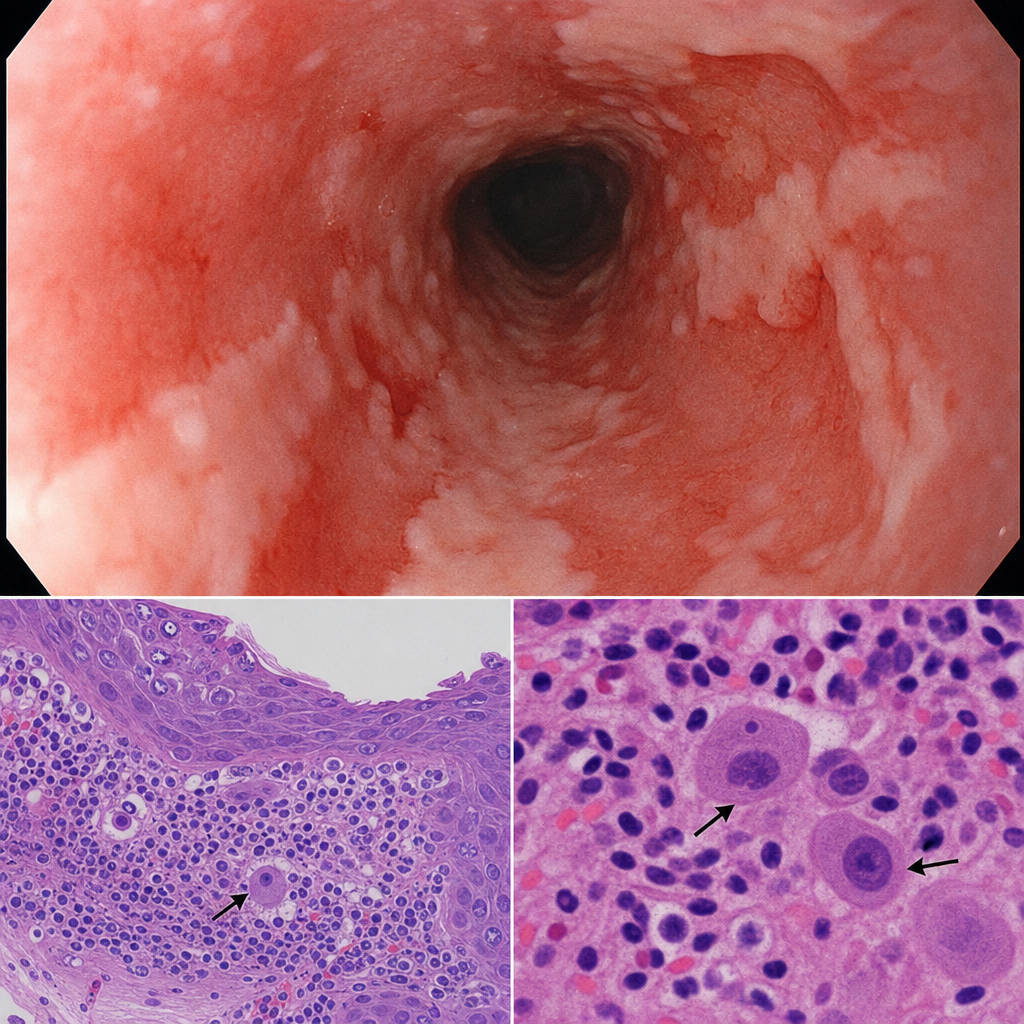
A 40-year-old immunocompromised patient presented with complaints of dysphagia. Upper GI scopy showed multiple ulcers in the distal esophagus. Biopsy from the esophagus showed specific findings. What is the diagnosis?
All of the following are true regarding Menetrier's disease, except:
Gastric carcinoma is associated with all EXCEPT:
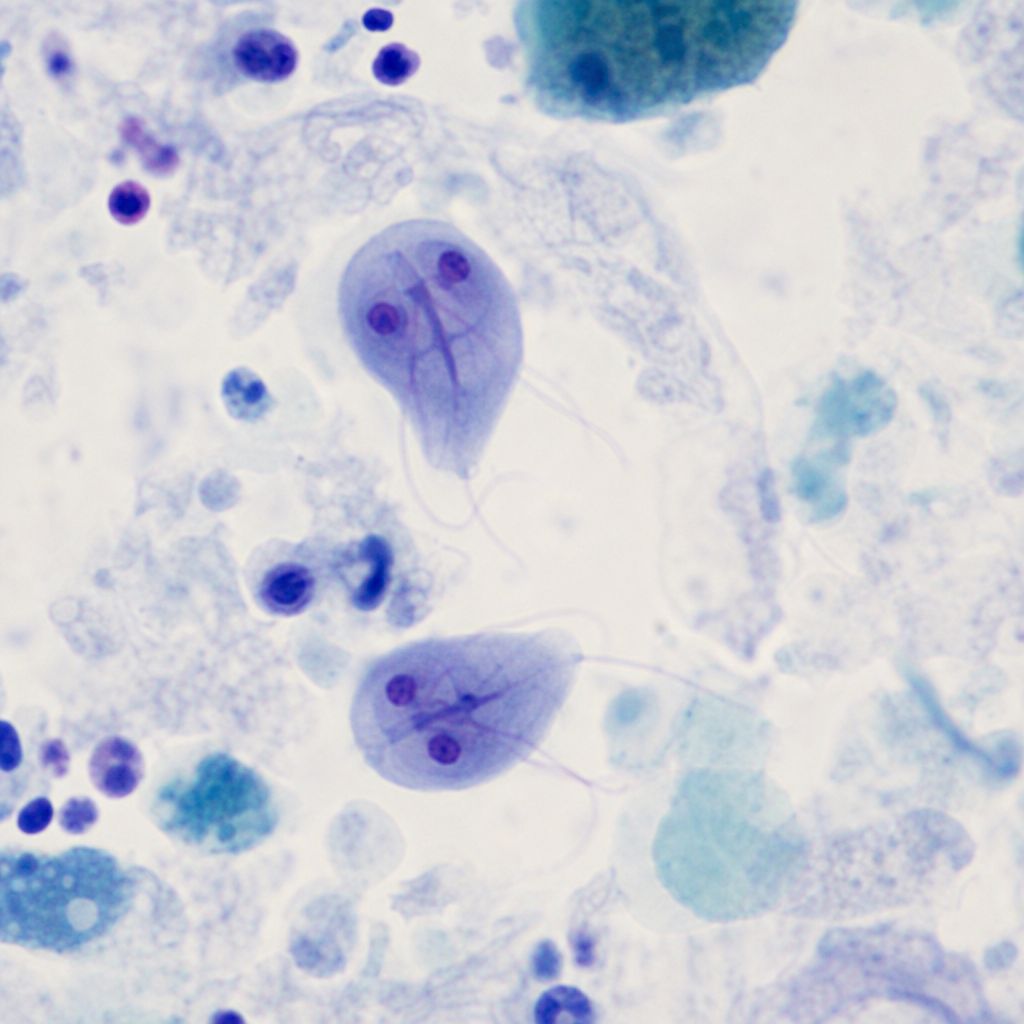
A patient presents with complaints of chronic diarrhea, accompanied by significant weight loss. An intestinal biopsy revealed specific findings. What is your diagnosis?
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app