
Gastrointestinal Pathology — MCQs

On this page
On histopathological examination of the gastro-esophageal junction, the following image is observed. What is the probable diagnosis?
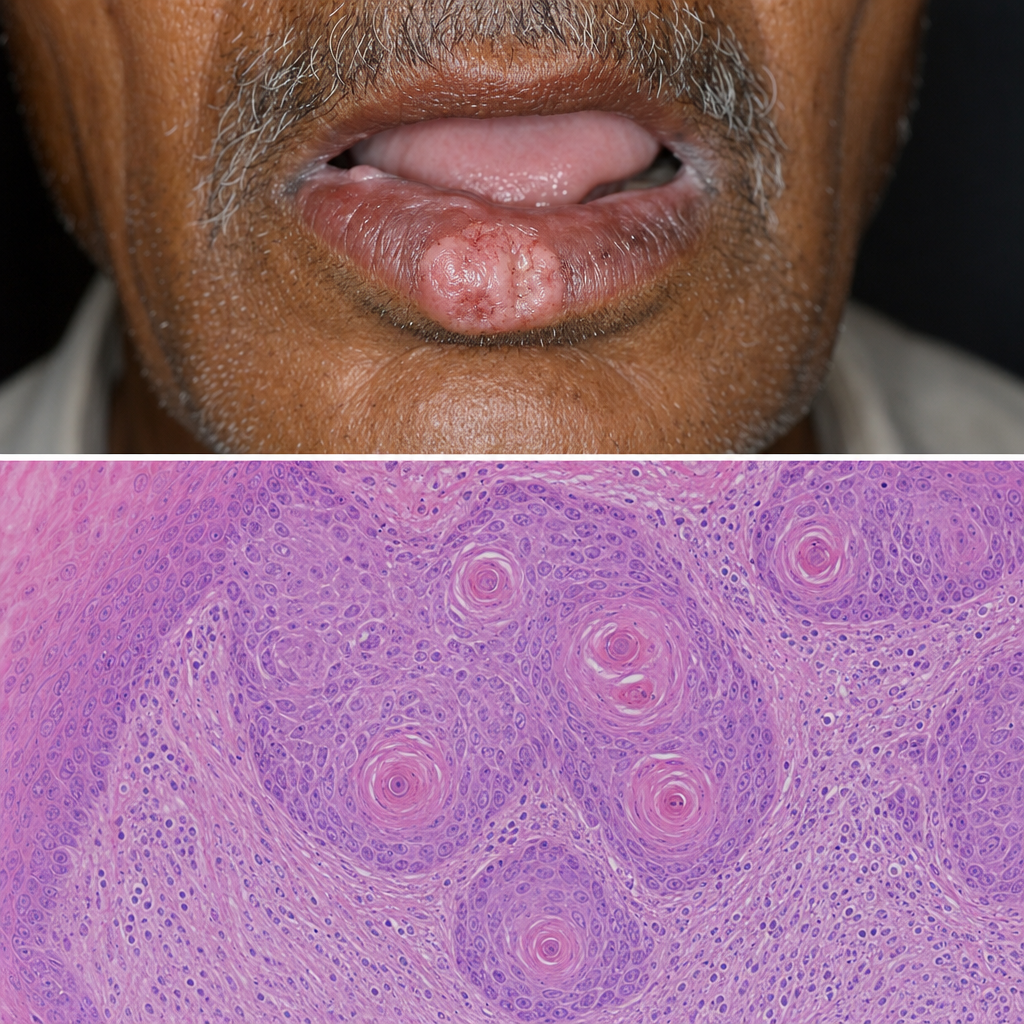
A 60-year-old male chronic smoker presents with a non-healing ulcer on the lower lip for 4 months. The lesion has raised everted edges and an indurated base. A biopsy is taken from the edge of the ulcer. The histology is shown in Image 1. Which of the following best describes the structural feature that most directly demonstrates squamous differentiation of this neoplasm?
A genetic study identifies a family with multiple members having early-onset colorectal cancer. DNA mismatch repair gene testing reveals a mutation in MLH1 gene. Which molecular phenomenon would be most prominently observed in tumor cells from these patients?
A 28-year-old man presents with difficulty swallowing solids and liquids for 2 years. Esophageal manometry shows aperistalsis in the distal esophagus and incomplete lower esophageal sphincter (LES) relaxation with wet swallows. Resting LES pressure is 45 mmHg (normal 10-30 mmHg). What is the underlying pathophysiologic defect?
What is the most common neoplasm of the appendix?
What is the most common site for leiomyoma in the gastrointestinal tract?
Which of the following conditions is not considered a premalignant condition?
Which of the following is true regarding pleomorphic adenoma?
Skip lesions are seen in which of the following conditions?
True about primary gastric lymphoma is
Practice by Chapter
Oral Cavity and Esophageal Pathology
Practice Questions
Gastritis and Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Vascular Disorders of Intestine
Practice Questions
Diverticular Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Infections
Practice Questions
Polyps and Neoplasms
Practice Questions
Appendiceal Pathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app