
Forensic Pathology — MCQs

On this page
All of the following are TRUE regarding myoglobinuria, EXCEPT:
A 25-year old patient who had a Road traffic accident was initially conscious but later became unconscious and subsequently died. On postmortem examination, multiple petechial hemorrhages are seen in the corpus callosum, what is the probable diagnosis?
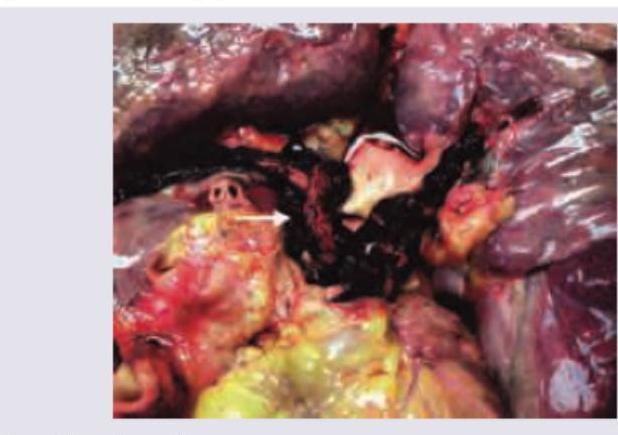
A 22-year-old biker had a road traffic accident with bilateral tibia fracture. After 7 days, his condition suddenly worsens and leads to death. Pathological specimen is provided. What could be the likely cause of death?
What is the Virchow method of organ removal in autopsy?
Practice by Chapter
Death Investigation
Practice Questions
Postmortem Changes
Practice Questions
Forensic Traumatology
Practice Questions
Asphyxial Deaths
Practice Questions
Thermal Injuries
Practice Questions
Gunshot and Explosive Injuries
Practice Questions
Forensic Toxicology
Practice Questions
Identification of Unknown Remains
Practice Questions
Sexual Assault Investigation
Practice Questions
Medicolegal Autopsy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app