
Thyroid Gland Diseases — MCQs

Metastases from follicular carcinoma should be treated by:
Radiation exposure can lead to which type of thyroid carcinoma?
A female presents with a 1 × 1 cm thyroid swelling. What is the next best step in management?
A 26-year-old male presents to the outpatient department with a discrete thyroid swelling. On neck ultrasound, an isolated cystic swelling of the gland is seen. What is the risk of malignancy associated with this finding?
A 40F presents with double vision, headaches, and a progressively enlarging thyroid mass. She has proptosis and limited eye movement. TSH is suppressed. Likely cause of her symptoms?
A 30-year-old woman presents with thyroid swelling. On investigations, her TSH levels are found to be elevated. Postoperative reports showed lymphocytic infiltration and Hurthle cells. A most probable diagnosis is?
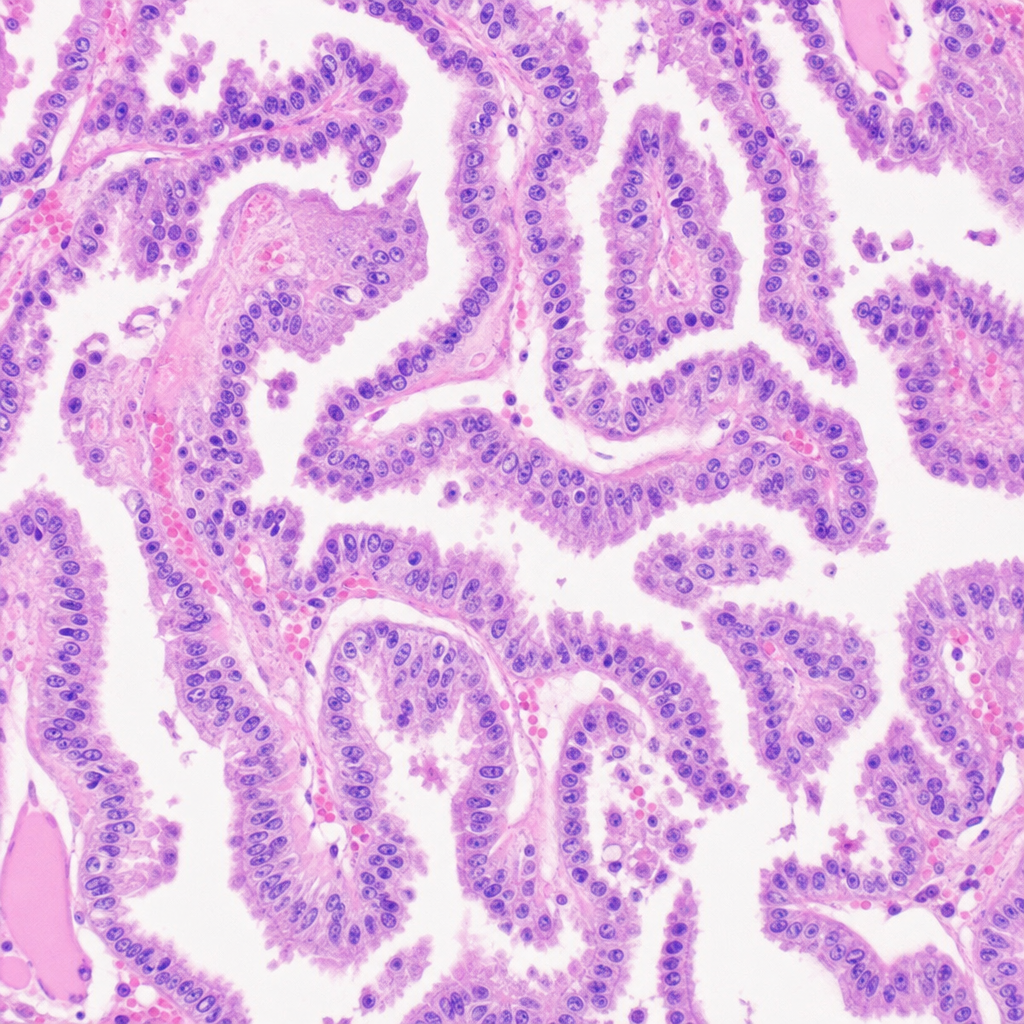
A 25-Year-old male presented with a 2cm thyroid nodule. A thyroidectomy was done. The histology picture is given below. What could be the diagnosis?
A 30-year-old female complaints of fatigue and is unable to gain weight. On examination, her body felt warm. Which of the following investigation can be helpful in reaching the diagnosis?
A 30-year-old came with complaints of thyroid swelling. On investigations her TSH levels were found to be elevated. Post-operative histopathological examination reports show lymphocytic infiltration and Hürthle cells. Which of the following is the most likely diagnosis?
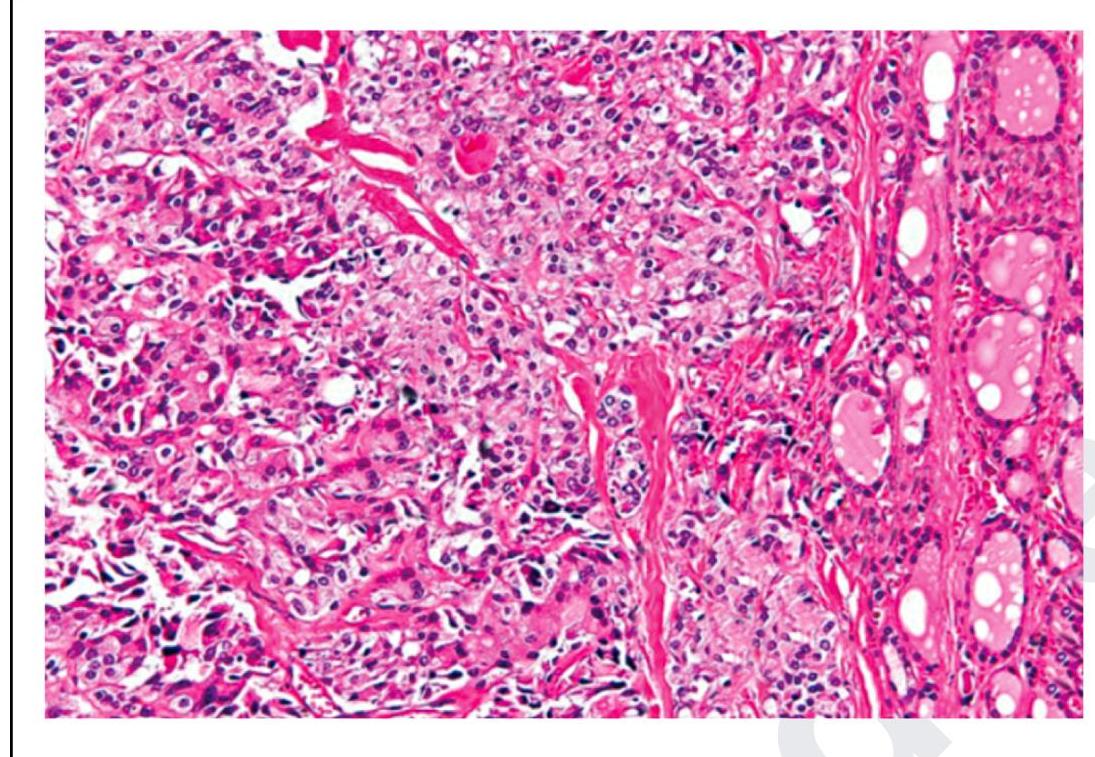
The following is a histopathological image of thyroid pathology. What is the diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app