
Pineal Gland Pathology — MCQs

All of the following are small round blue cell tumours except
A 42-year-old man complains of head¬ache when he wakes up in the morning. It lasts into the afternoon and then subsides. Headache has been present for a few months. CT scan shows a frontal lobe mass with focal areas of calcification. You strongly suspect the pa¬tient has
Which of the following is the ovarian counterpart of testicular seminoma?
Craniopharyngioma arises from -
Hormonal secretions are tightly controlled by the time of day due to an inbuilt biological clock in human body. This rhythmic secretion is controlled by:
A 30-year-old woman presents with a history of amenorrhea and impaired vision of six months' duration. Physical examination shows normal findings except for pale optic discs and diminished visual acuity. The most likely diagnosis is -
Most radiosensitive tumor among the following is
Which of the following testicular tumors is not a germ cell neoplasm?
Melatonin is secreted from which cells of pineal gland?
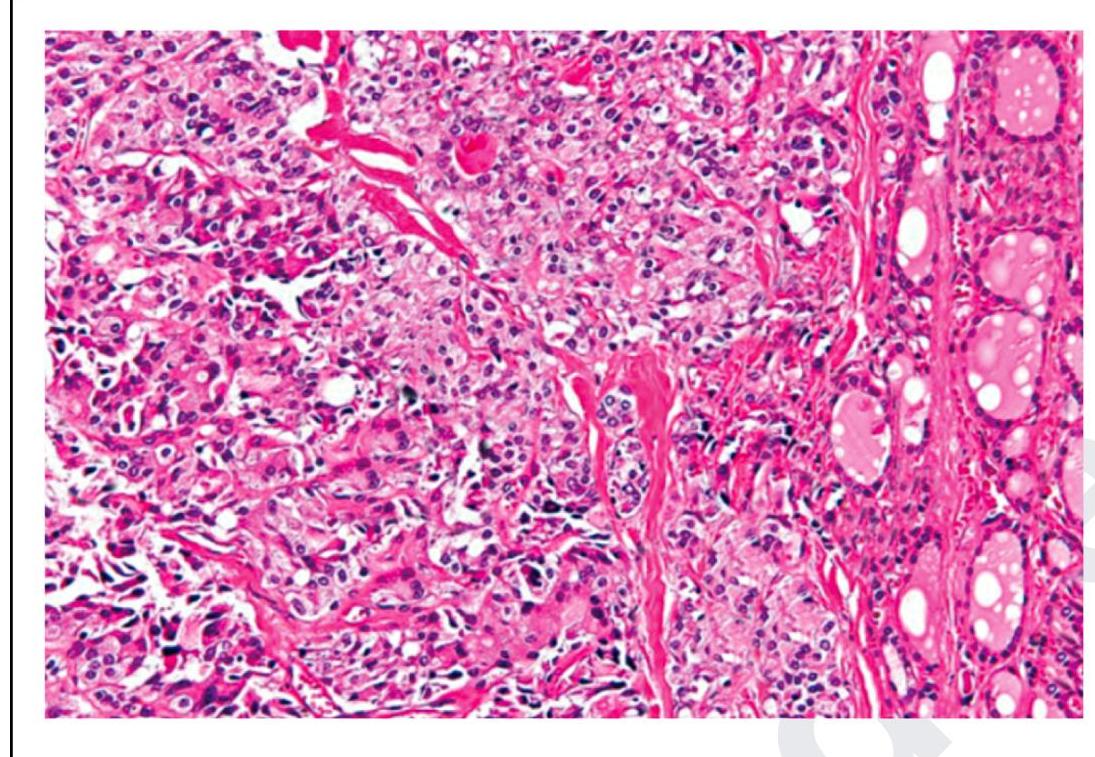
The following is a histopathological image of thyroid pathology. What is the diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app