
Parathyroid Gland Pathology — MCQs

The function of which of the following is increased by an elevated parathyroid hormone concentration:
Hypophosphatemia is seen in:
The commonest cause of primary hyperparathyroidism is what?
All are true about primary hyperparathyroidism except which of the following?
Hypocalcemia in a child may be associated with
Primary Hyperparathyroidism is associated with -
Primary hyperparathyroidism is suggested by all of the following, except which of the following?
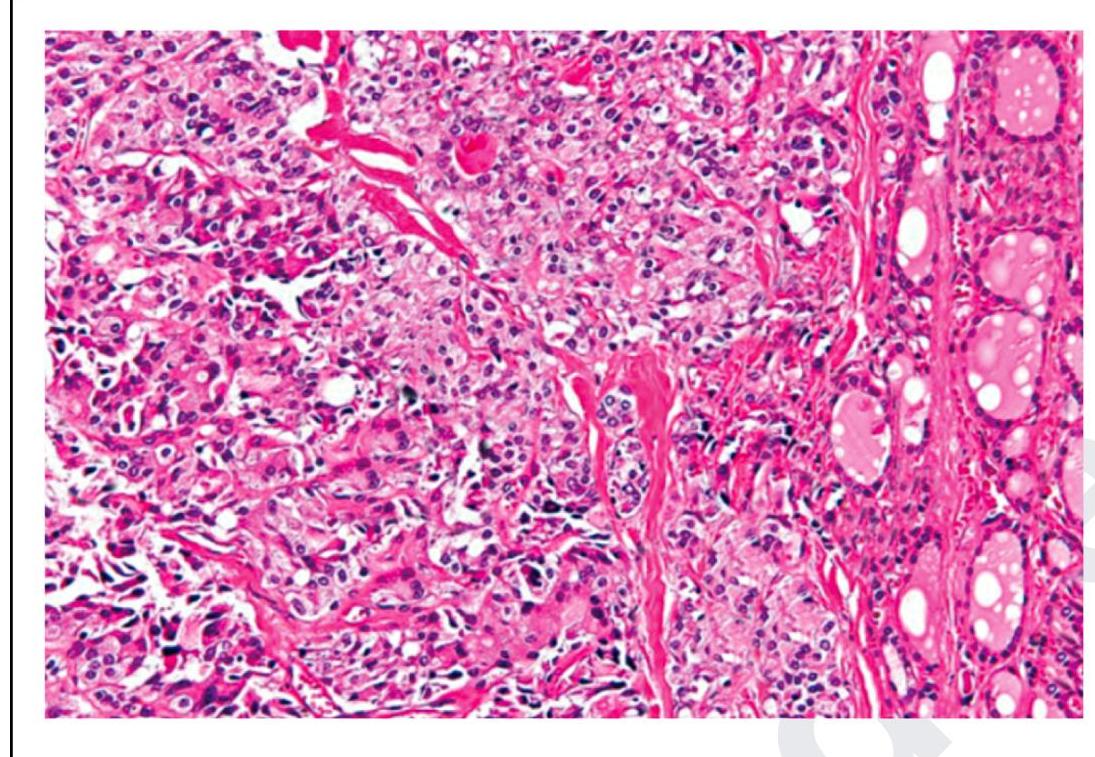
The following is a histopathological image of thyroid pathology. What is the diagnosis?
Chvostek sign could be seen after -
Most sensitive investigation for preoperative localization of abnormal parathyroid glands is
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app