
Endocrine Pathology — MCQs

On this page
A 42-year-old woman presents with a diffuse swelling in front of her neck. Thyroid function tests are within normal limits. A fine-needle biopsy reveals malignant cells. On examination of the excised tumor, the tumor cells are positive for calcitonin on immunohistochemistry. What is the appropriate pathologic diagnosis?
Which of the following is NOT a true statement about papillary carcinoma?
A 27-year-old female presented with a long-standing 2 cm x 2 cm nodule in the right lobe of her thyroid, for which she underwent a right hemithyroidectomy. What is the most likely histopathological finding given these clinical details?
What is the pathognomic feature of hyperparathyroidism?
A 25-year-old man presents with 3 months of polyuria and increased thirst. The patient suffered trauma to the base of the skull in a motorcycle accident 4 months ago. A 24-hour urine collection shows polyuria but no evidence of hematuria, glucosuria, or proteinuria. The pathogenesis of polyuria in this patient is most likely caused by a lesion in which of the following areas of the brain?
What is the most common cause of primary hyperparathyroidism?
Compared to follicular carcinoma, papillary carcinoma of the thyroid is associated with which of the following?
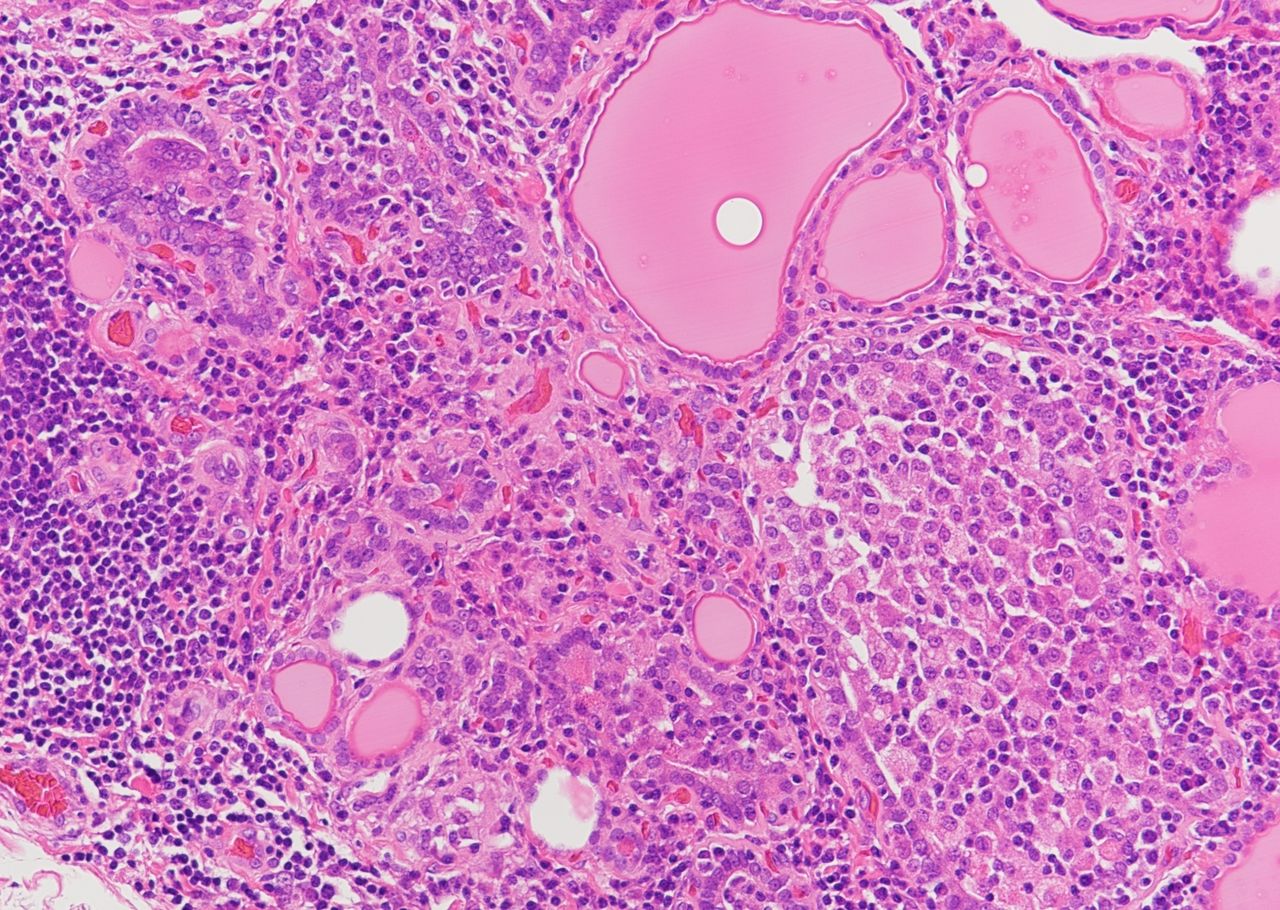
A 45-year-old female patient presented with features of hypothyroidism. Based on the provided histological features, what is your diagnosis?
All are seen in MEN IIA syndrome except?
Pancreatitis, pituitary tumor, and pheochromocytoma may be associated with which of the following types of thyroid cancer?
Practice by Chapter
Pituitary Gland Disorders
Practice Questions
Thyroid Gland Diseases
Practice Questions
Parathyroid Gland Pathology
Practice Questions
Adrenal Cortical Disorders
Practice Questions
Adrenal Medullary Disorders
Practice Questions
Pancreatic Endocrine Disorders
Practice Questions
Multiple Endocrine Neoplasia Syndromes
Practice Questions
Diffuse Neuroendocrine System
Practice Questions
Pineal Gland Pathology
Practice Questions
Laboratory Diagnosis of Endocrine Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app