
Endocrine Pathology — MCQs

On this page
Regarding anaplastic thyroid carcinoma, which of the following statements is true?
Radiation exposure can lead to which type of thyroid carcinoma?
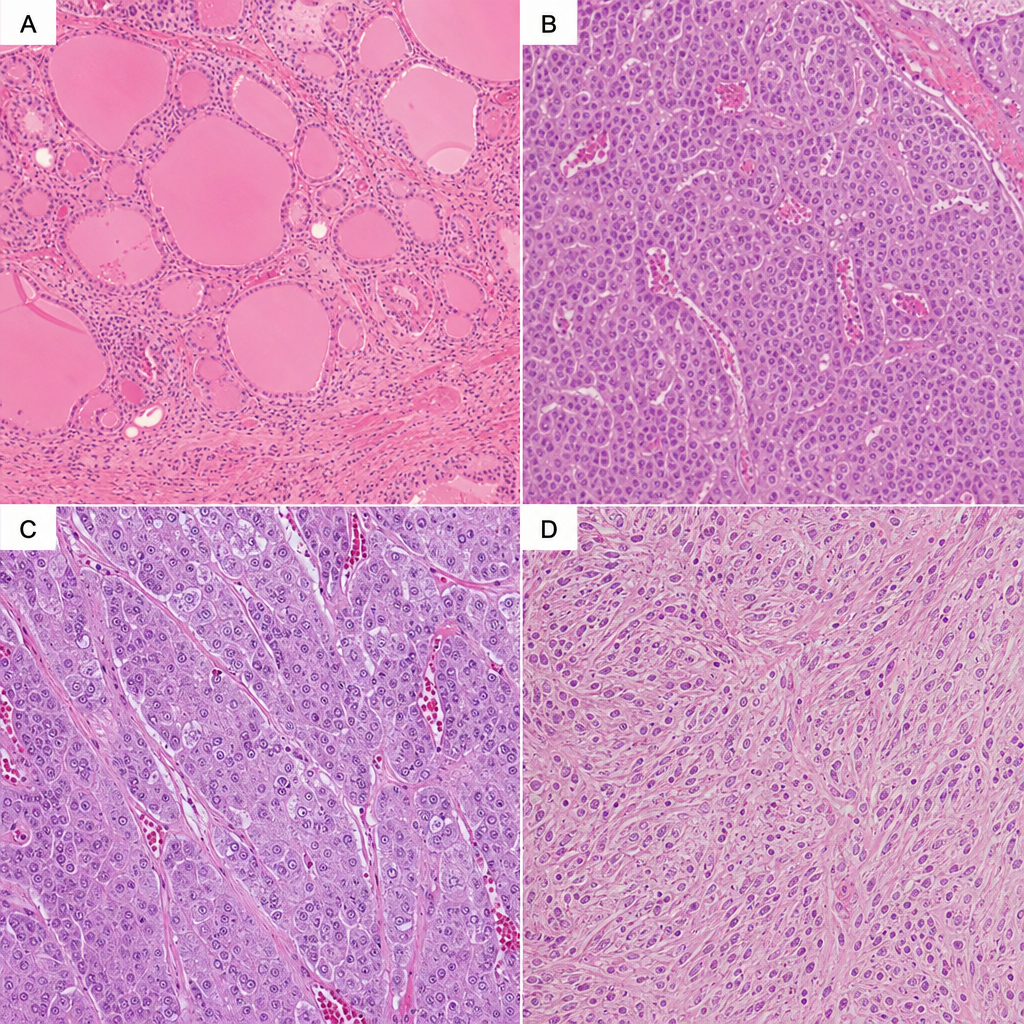
A 65-year-old female patient presented with complaints of a swelling in the neck which moved with deglutition along with multiple episodes of diarrhea, hoarseness, mild dysphagia and mild shortness of breath. Lab findings revealed raised serum calcitonin levels and hypercalcemia. Which of the following histology corresponds with the above disease?
A well-differentiated follicular carcinoma of the thyroid can be best differentiated from a follicular adenoma by:
What is the key histological feature that differentiates follicular carcinoma from follicular adenoma of the thyroid?
Malignancy in pheochromocytoma is indicated by:
Mark the false statement regarding Hürthle cell carcinoma:
All the following statements about thyroid carcinoma are true, except which one?
The expression of which gene is most strongly associated with a high incidence of medullary carcinomas of the thyroid?
Practice by Chapter
Pituitary Gland Disorders
Practice Questions
Thyroid Gland Diseases
Practice Questions
Parathyroid Gland Pathology
Practice Questions
Adrenal Cortical Disorders
Practice Questions
Adrenal Medullary Disorders
Practice Questions
Pancreatic Endocrine Disorders
Practice Questions
Multiple Endocrine Neoplasia Syndromes
Practice Questions
Diffuse Neuroendocrine System
Practice Questions
Pineal Gland Pathology
Practice Questions
Laboratory Diagnosis of Endocrine Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app