
Endocrine Pathology — MCQs

On this page
A 5-year-old child presents with a large abdominal mass and hypertension. Histology reveals small round blue cells and Homer-Wright rosettes. What is the most likely diagnosis?
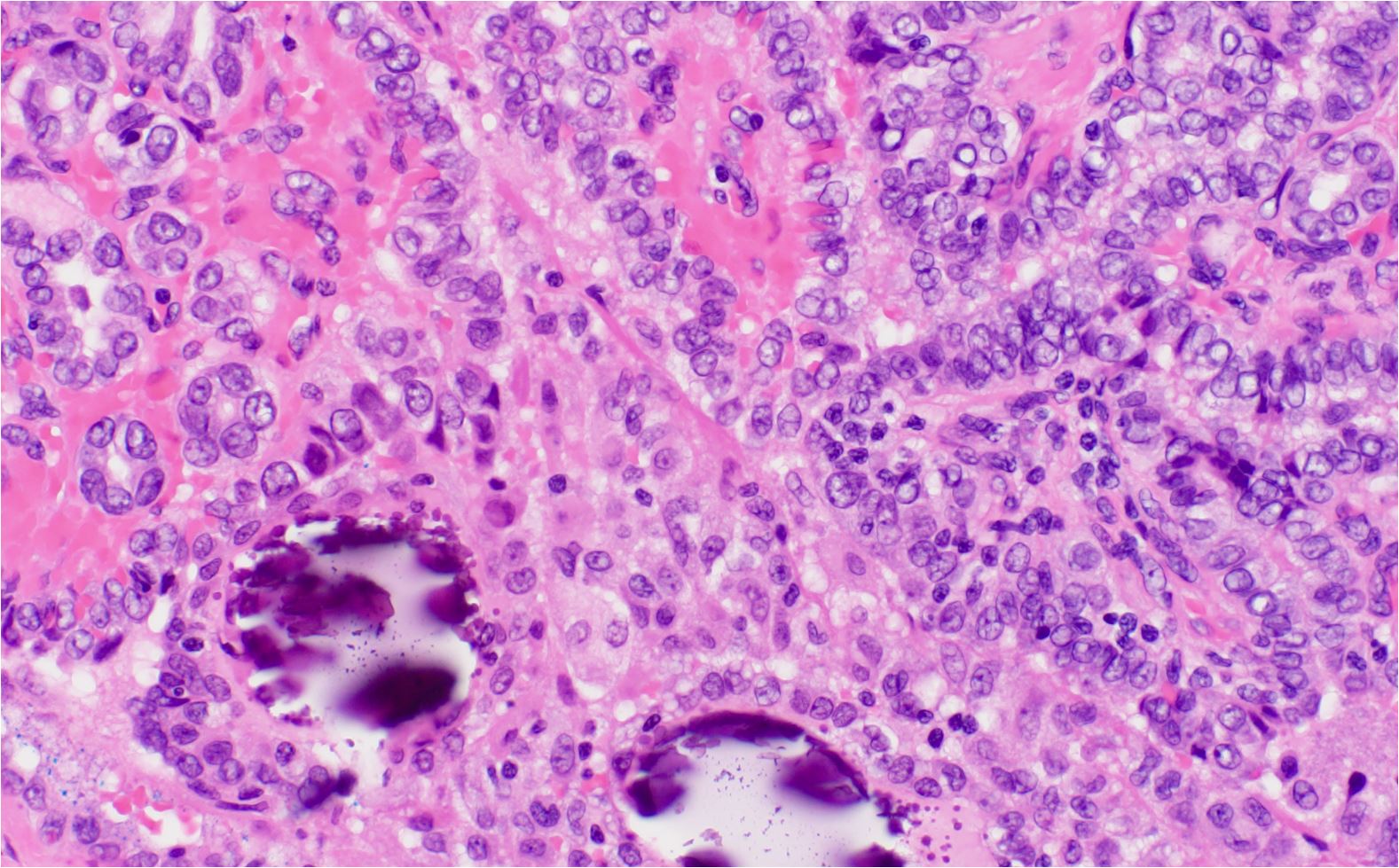
A thyroid nodule biopsy reveals cells with nuclear overlapping and a papillary architecture. Which molecular alteration is most commonly associated with this condition?
A 67-year-old woman with hypertension and diabetes presents with a painless neck mass. Fine-needle aspiration biopsy reveals spindle-shaped cells. What is the most likely diagnosis?
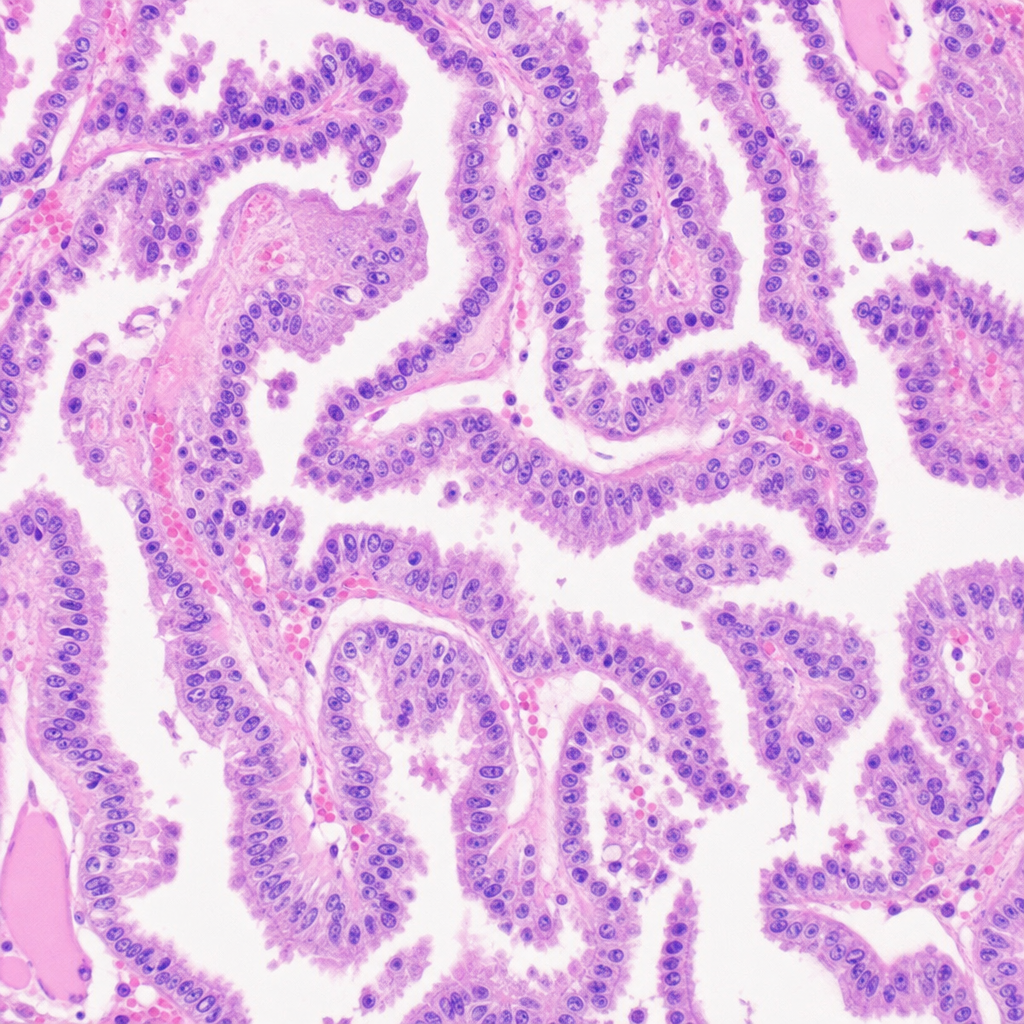
A 25-Year-old male presented with a 2cm thyroid nodule. A thyroidectomy was done. The histology picture is given below. What could be the diagnosis?
Which of the following is true about the development of thyroid tumors in nodular goiter?
Which HLA marker is associated with an increased risk of developing type 1 diabetes mellitus?
Sheehan syndrome is?
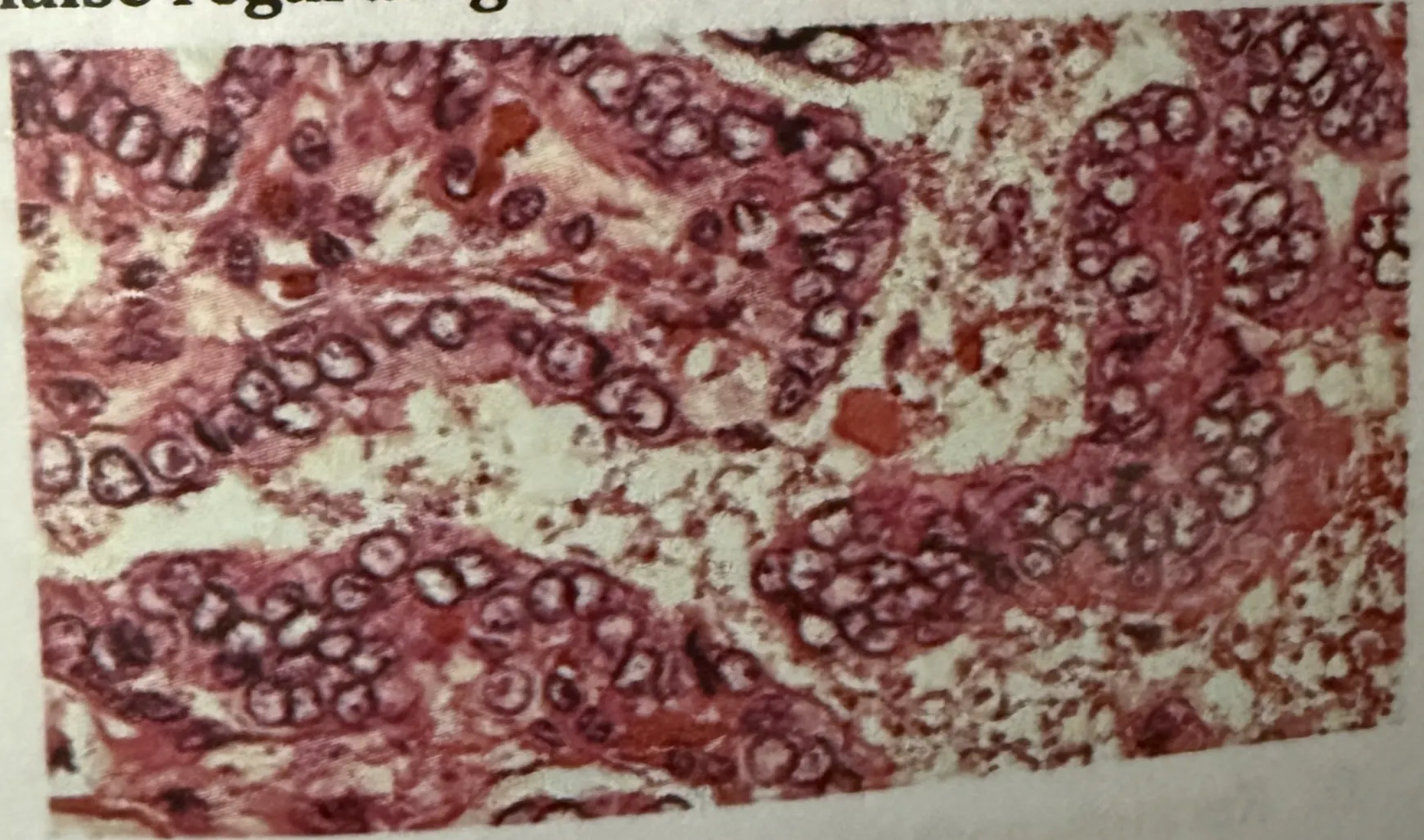
A middle aged male patient presents with painless slow growing neck swelling. On examination, lymph nodes are positive. Surgery is done and biopsy is shown in the image below. Which of the following is false regarding the HPE findings?
A 25-year-old male presented with a 2cm thyroid nodule. A thyroidectomy was done. The histology picture is given below. What could be the diagnosis based on the histological findings?
A 30-year-old woman presents with thyroid swelling. On investigations, her TSH levels are found to be elevated. Postoperative reports showed lymphocytic infiltration and Hurthle cells. A most probable diagnosis is?
Practice by Chapter
Pituitary Gland Disorders
Practice Questions
Thyroid Gland Diseases
Practice Questions
Parathyroid Gland Pathology
Practice Questions
Adrenal Cortical Disorders
Practice Questions
Adrenal Medullary Disorders
Practice Questions
Pancreatic Endocrine Disorders
Practice Questions
Multiple Endocrine Neoplasia Syndromes
Practice Questions
Diffuse Neuroendocrine System
Practice Questions
Pineal Gland Pathology
Practice Questions
Laboratory Diagnosis of Endocrine Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app