
Endocrine Pathology — MCQs

On this page
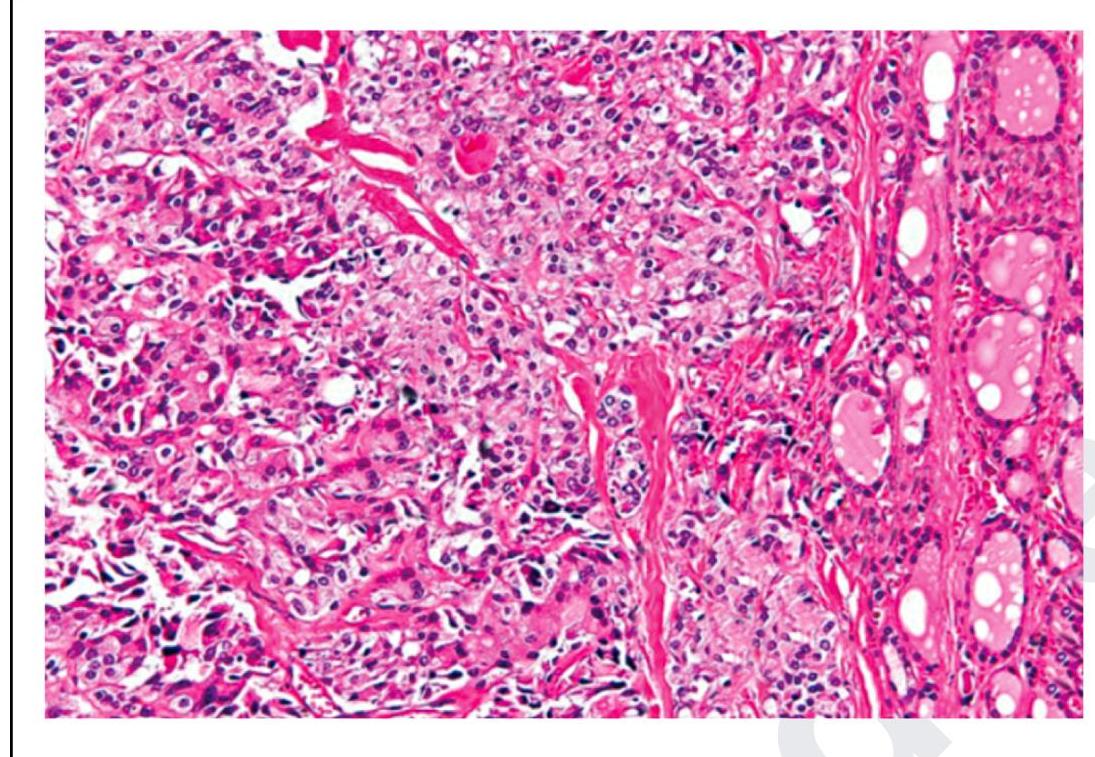
A patient presents with headaches, palpitations, hypertension, and urine VMA positivity. The biopsy findings are shown in the image. Which of the following statements is correct?
The following is a histopathological image of thyroid pathology. What is the diagnosis?
A thyroid FNA shows 'bubble gum' colloid. Which nuclear feature would best support papillary thyroid carcinoma?
Pheochromocytoma produces all except?
Malignancy in a multinodular goiter is most often:-
Pseudohermaphroditism (Disorder of Sex Development - DSD) is most commonly seen with which tumor?
Nesidioblastoma is due to hyperplasia of?
A 14-year-old male presents with type I diabetes mellitus. His mother wants to know if the boy's brother might also have an increased risk of getting the disease. Which of the following genotypes, if present in the brother, would be associated with the greatest risk of developing diabetes?
Neuroblastoma originates from –
Which of the following occurs in long standing goitre:
Practice by Chapter
Pituitary Gland Disorders
Practice Questions
Thyroid Gland Diseases
Practice Questions
Parathyroid Gland Pathology
Practice Questions
Adrenal Cortical Disorders
Practice Questions
Adrenal Medullary Disorders
Practice Questions
Pancreatic Endocrine Disorders
Practice Questions
Multiple Endocrine Neoplasia Syndromes
Practice Questions
Diffuse Neuroendocrine System
Practice Questions
Pineal Gland Pathology
Practice Questions
Laboratory Diagnosis of Endocrine Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app