
Endocrine Pathology — MCQs

On this page
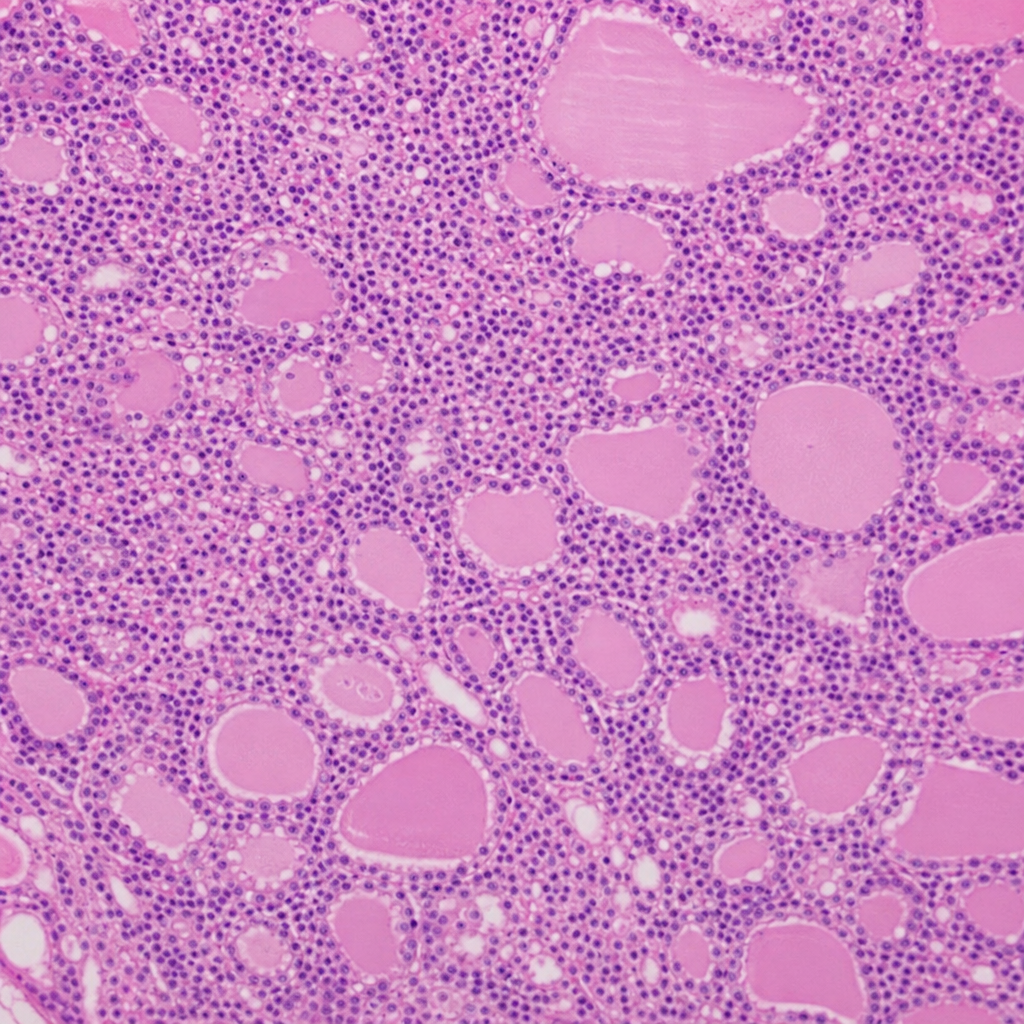
A 25-year-old female presented with features of weight gain, loss of appetite, and easy fatigue. On examination, a swelling was noticed in the anterior aspect of the neck which moved with deglutition. A biopsy performed from the neck revealed characteristic findings. What is your diagnosis?
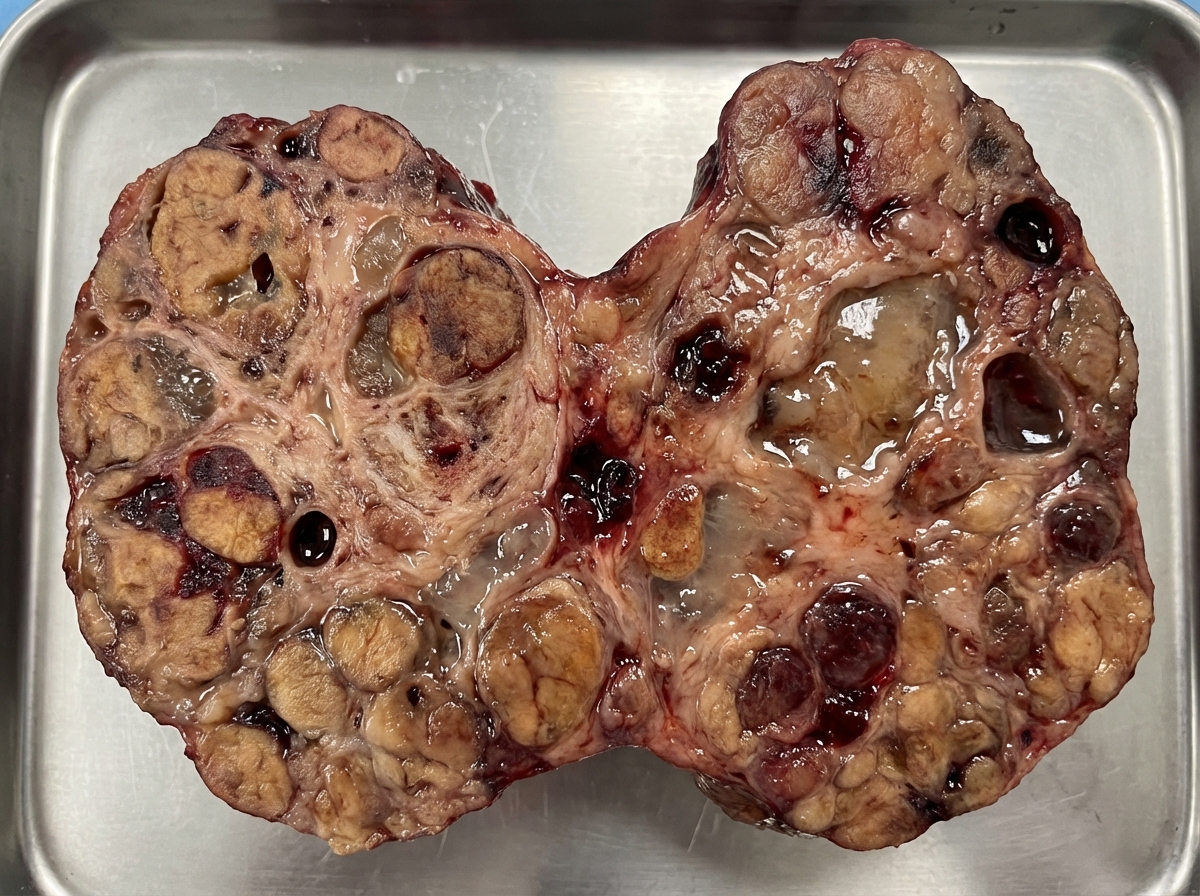
The specimen shown below is:
Which gene is involved in the pathogenesis of Type 1 Diabetes mellitus?
Which type of adenoma has the highest propensity to undergo dystrophic calcification?
A 29-year-old woman presents with a 6-month history of nervousness, muscle weakness, heat intolerance, excessive sweating, and a 9 kg weight loss despite increased caloric intake. She also reports palpitations and amenorrhea. Physical examination reveals warm, moist skin and exophthalmos. A thyroid biopsy is performed. Which of the following best describes the expected pathologic findings?
Pheochromocytoma with malignant potential exclusively secretes which of the following?
Familial hypocalciuric hypercalcemia is characterized by mild elevation of calcium and parathyroid hormone (PTH) levels. It is primarily caused by a mutation in which of the following?
A 56-year-old woman presents with a 7-month history of an enlarging lump on the right side of her neck. Physical examination reveals a 3-cm nodule in the right upper neck, medial to the sternocleidomastoid muscle and lateral to the trachea, at the angle of the mandible. A CT scan shows a circumscribed, solid mass adjacent to the carotid bifurcation. Microscopic examination of the excised mass reveals nests of round cells with pink, granular cytoplasm. Immunohistochemical markers chromogranin and S-100 are positive. Electron microscopy shows neurosecretory granules in the tumor cell cytoplasm. The tumor recurs 1 year later and is re-excised. What is the most likely diagnosis?
A tumor similar to that shown in the illustration is observed in a biopsy specimen from the thyroid of a 50-year-old woman. An adjacent lymph node is also involved. Which of the following descriptions of this tumor is most appropriate?
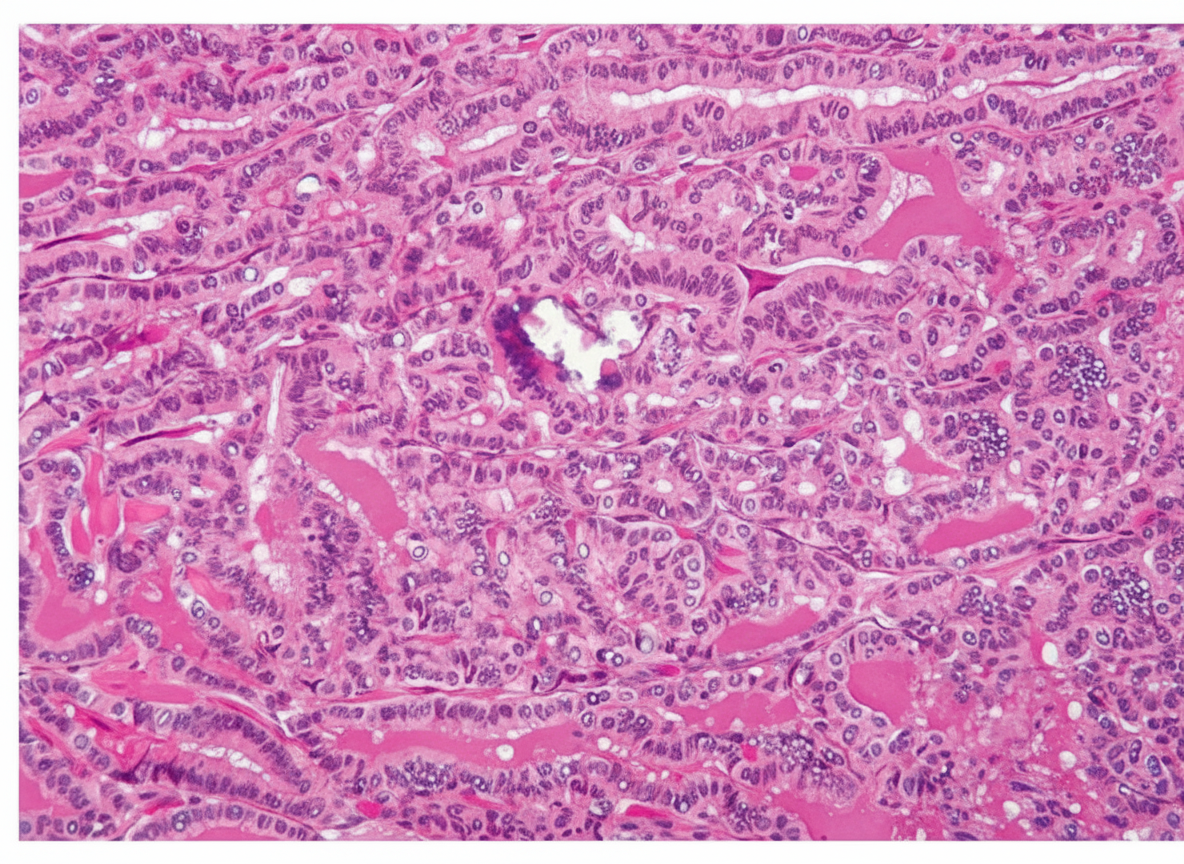
A 38-year-old woman undergoes a subtotal thyroidectomy. The biopsy specimen contains psammoma bodies and prominent papillae of epithelium with a fibrovascular core. The nuclear region of the cells shows groove formation, optical clearing, eosinophilic inclusions, and overlapping of nuclei. Which of the following is the most likely diagnosis?
Practice by Chapter
Pituitary Gland Disorders
Practice Questions
Thyroid Gland Diseases
Practice Questions
Parathyroid Gland Pathology
Practice Questions
Adrenal Cortical Disorders
Practice Questions
Adrenal Medullary Disorders
Practice Questions
Pancreatic Endocrine Disorders
Practice Questions
Multiple Endocrine Neoplasia Syndromes
Practice Questions
Diffuse Neuroendocrine System
Practice Questions
Pineal Gland Pathology
Practice Questions
Laboratory Diagnosis of Endocrine Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app