
Endocrine Pathology — MCQs

On this page
Which of the following statements about pheochromocytoma is incorrect?
Persistent multinodular goiter may cause which of the following complications?
Which is the most well-differentiated thyroid tumor?
Medullary thyroid carcinoma occurs due to the mutation of which oncogene or gene?
All of the following are features of De Quervain thyroiditis except?
A 32-year-old woman develops an Addisonian crisis (acute adrenal insufficiency) 3 months after suffering massive hemorrhage during the delivery of her baby. A CT scan of the abdomen shows small adrenal glands. Which of the following mechanisms of disease best accounts for adrenal atrophy in this patient?
Multiple Endocrine Neoplasia (MEN) types II and III are associated with which gene mutation?
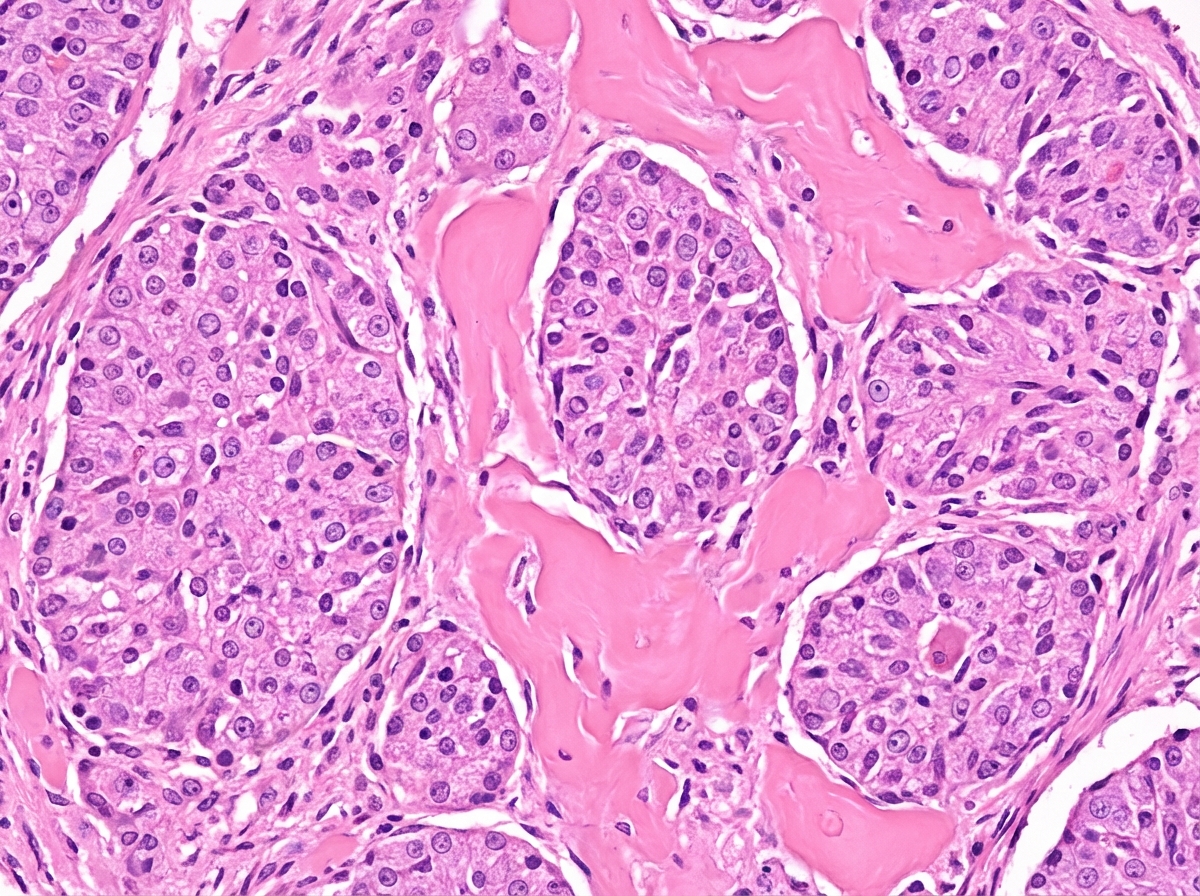
A 40-year-old male presented with a thyroid swelling and dysphagia. He gave history of on and off watery diarrhea. Biopsy of the lesion is shown. What is your diagnosis?
Which of the following is seen on electron microscopy of medullary thyroid carcinoma specimens?
What is the ultrastructural finding in a case of paraganglioma?
Practice by Chapter
Pituitary Gland Disorders
Practice Questions
Thyroid Gland Diseases
Practice Questions
Parathyroid Gland Pathology
Practice Questions
Adrenal Cortical Disorders
Practice Questions
Adrenal Medullary Disorders
Practice Questions
Pancreatic Endocrine Disorders
Practice Questions
Multiple Endocrine Neoplasia Syndromes
Practice Questions
Diffuse Neuroendocrine System
Practice Questions
Pineal Gland Pathology
Practice Questions
Laboratory Diagnosis of Endocrine Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app