
Diffuse Neuroendocrine System — MCQs

Which of the following cells in the lungs are classified as neuroendocrine cells?
VIPoma is associated with which syndrome?
FDG-PET negative tumor is:
All of the following statements are true about Gleason score, except:
Submucosal neuroma is associated with
Which of the following glands is NOT involved in Type I MEN?
MC location of gastrinoma in MEN-1 syndrome?
What is the most common type of acute myeloid leukemia in patients with Down's syndrome?
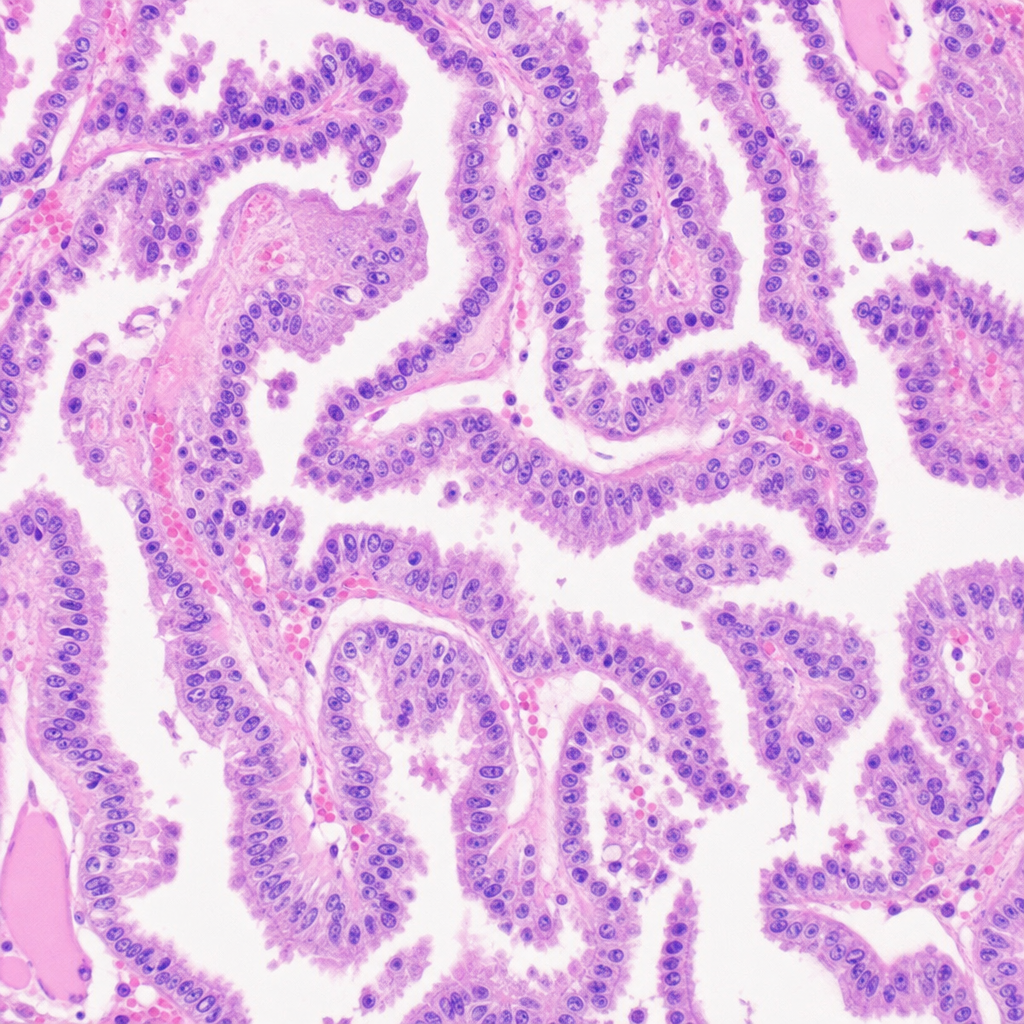
A 25-Year-old male presented with a 2cm thyroid nodule. A thyroidectomy was done. The histology picture is given below. What could be the diagnosis?
A 28-year-old woman has noticed increasing lower limb swelling and shortness of breath, with a 2-year history of facial rash, hair loss, arthralgias, and thrombocytopenia. On examination, her blood pressure is 150/90 mmHg, pulse 80/min, with a maculopapular rash on her face, JVP of 4 cm, normal heart sounds, clear lungs, and pedal and periorbital edema. Her creatinine is very high, and a urinalysis reveals many RBCs and RBC casts. For this patient with glomerulonephritis, select the most likely diagnosis on renal biopsy.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app