
Cytopathology — MCQs

On this page
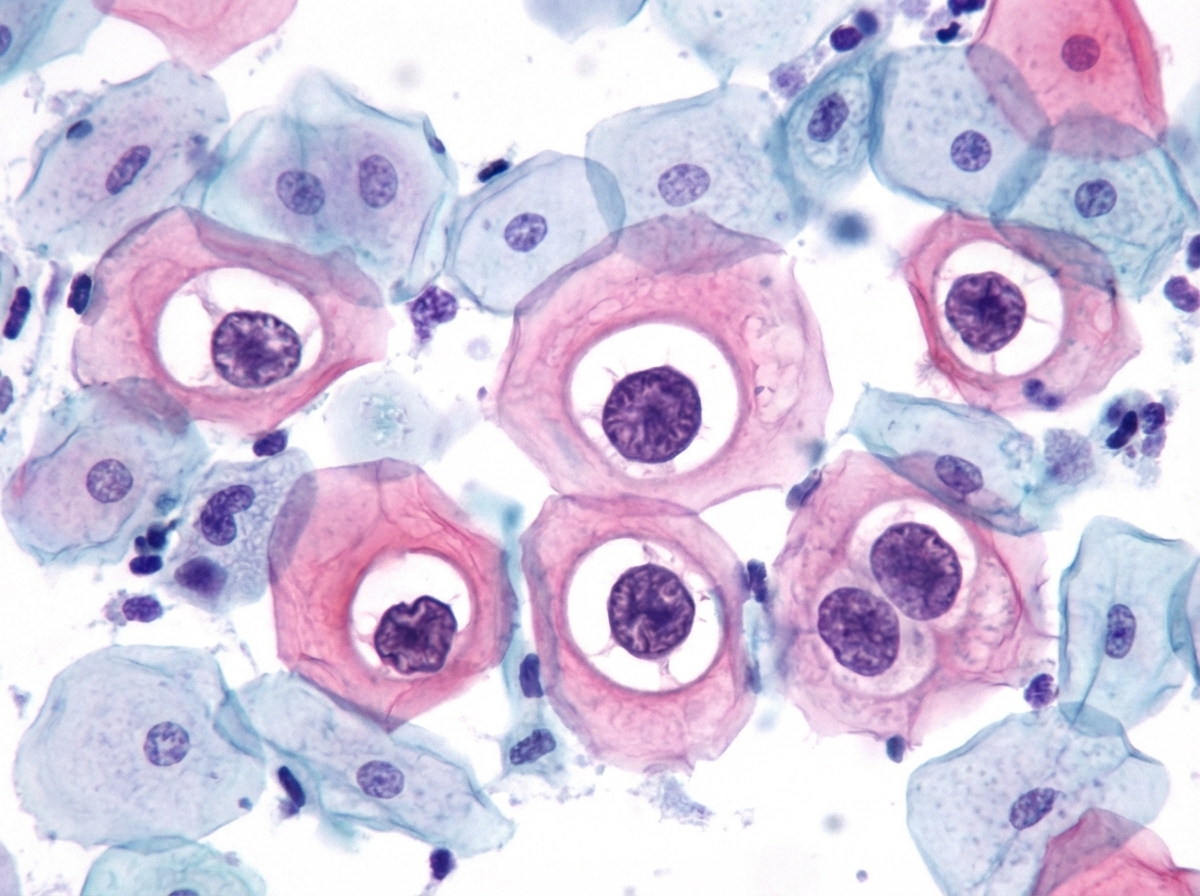
A 15-year-old girl undergoes Pap smear analysis. The smear demonstrates koilocytes, which are approximately the same size as intermediate cells, with enlarged hyperchromatic nuclei and perinuclear halos. These abnormal cells are infected by which of the following viruses?
A 75-year-old woman has experienced increasing dull but constant pain in the back, right chest, left shoulder, and left upper thigh for the past 6 months. She has now developed a sudden, severe, sharp pain in the left thigh. On physical examination, she has intense pain on palpation of the upper thigh, and the left leg is shorter than the right. A radiograph of the left leg shows a fracture through the upper diaphyseal region of the femur in a 5-cm lytic area that extends through the entire thickness of the bone. A bone scan shows multiple areas of increased uptake in the left femur, pelvis, vertebrae, right third and fourth ribs, upper left humerus, and left scapula. Laboratory studies show serum creatinine, 0.9 mg/dL; total protein, 6.7 g/dL; albumin, 4.5 g/dL; total bilirubin, 1 mg/dL; AST, 28 U/L; ALT, 22 U/L; and alkaline phosphatase, 202 U/L. What is the most likely diagnosis?
Based on the characteristic cytological findings on PAP smear examination in a 26-year-old female presented for screening, what is your diagnosis?
A 60-year-old female with a 8-year history of renal failure on hemodialysis develops Carpal Tunnel syndrome. Which of the following types of amyloid will be associated with this condition?
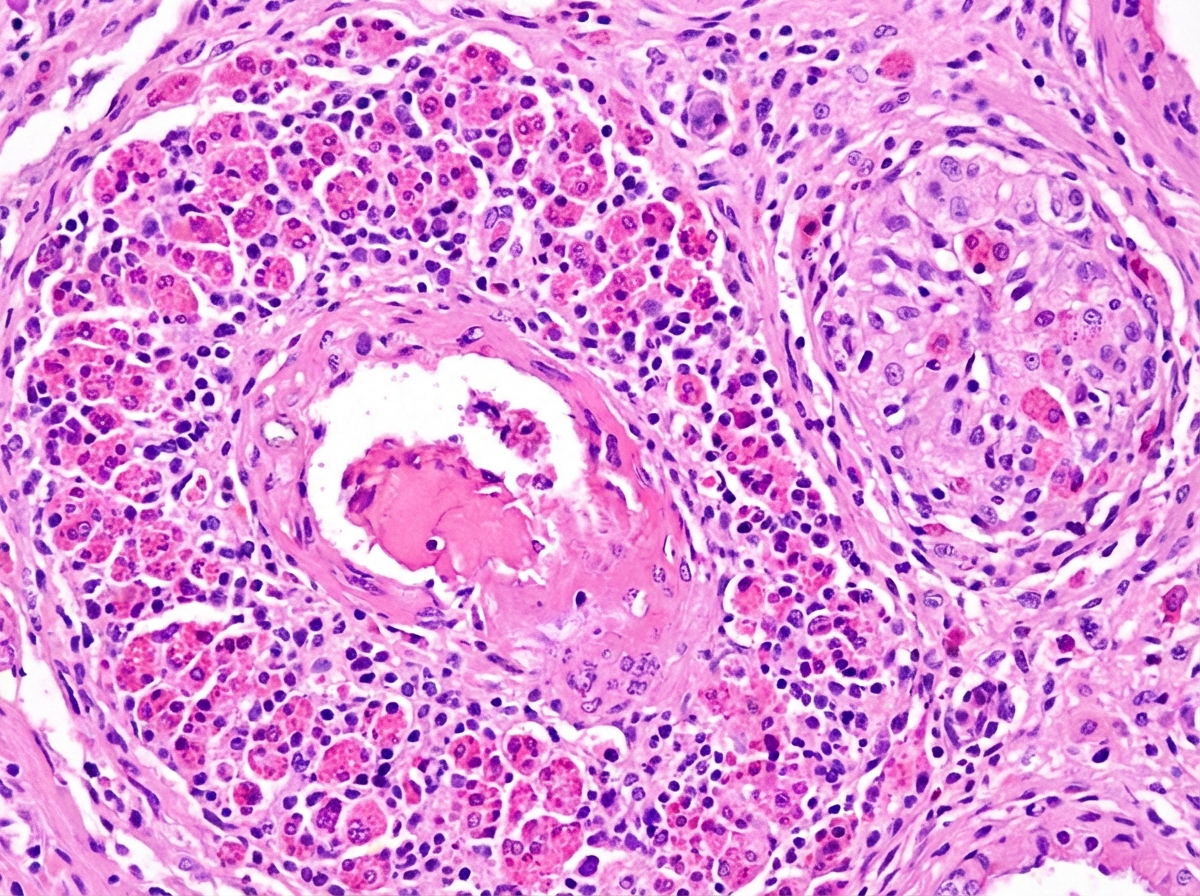
A 35-year-old patient presents with persistent allergic rhinitis, asthmatic episodes, and peripheral hypereosinophilia. Histological findings are shown below. What is your diagnosis?
Acridine orange is a fluorescent dye used to bind which cellular components?
FNAC is useful in diagnosing all the following conditions EXCEPT?
What is the best fixative for a Pap smear?
Regarding the screening of oral cancer, which of the following statements about exfoliative cytology is NOT true?
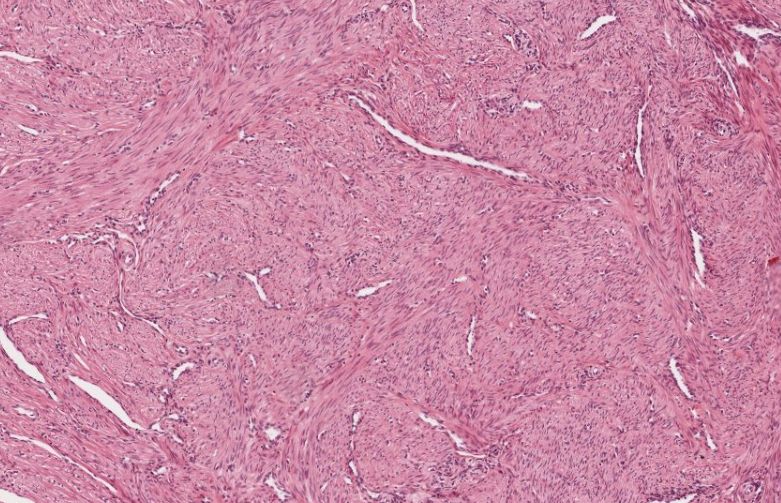
A 45-year-old female underwent hysterectomy for dysfunctional uterine bleeding. Following are the gross and histological findings. Which of the following is the most likely diagnosis?
Practice by Chapter
Basic Principles of Cytopathology
Practice Questions
Specimen Collection and Processing
Practice Questions
Gynecologic Cytology
Practice Questions
Respiratory Tract Cytology
Practice Questions
Urinary Tract Cytology
Practice Questions
Effusion Cytology
Practice Questions
Fine Needle Aspiration Cytology
Practice Questions
Gastrointestinal Tract Cytology
Practice Questions
Ancillary Studies in Cytopathology
Practice Questions
Quality Assurance in Cytopathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app