
Cytopathology — MCQs

On this page
In Pap smear cytology, which of the following is the most appropriate fixative used to preserve cellular details immediately after smearing?
Name the cell marked as X in Pap smear.
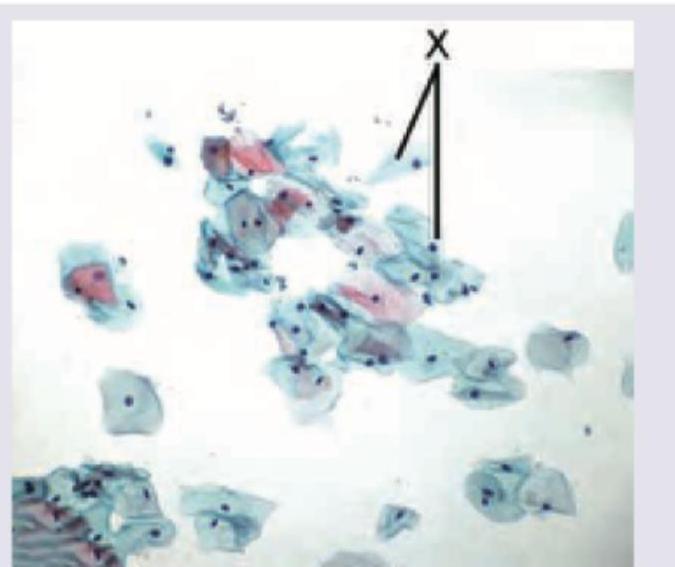
Name the cells marked as X in Pap smear.

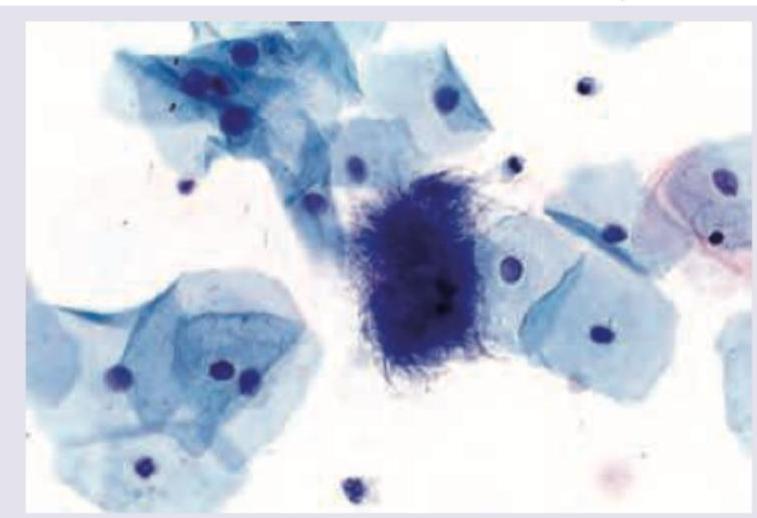
The following pap smear shows infestation by:
A woman on Pap smear shows disorganized growth of cells with hyperchromatic nuclei. Which phenomenon is occurring here?
Which of the following statements is correct regarding the use of histopathological examination techniques for mass screening of endometrial cancer?
Practice by Chapter
Basic Principles of Cytopathology
Practice Questions
Specimen Collection and Processing
Practice Questions
Gynecologic Cytology
Practice Questions
Respiratory Tract Cytology
Practice Questions
Urinary Tract Cytology
Practice Questions
Effusion Cytology
Practice Questions
Fine Needle Aspiration Cytology
Practice Questions
Gastrointestinal Tract Cytology
Practice Questions
Ancillary Studies in Cytopathology
Practice Questions
Quality Assurance in Cytopathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app