
Cytopathology — MCQs

On this page
A Pap smear is useful in the diagnosis of all the following EXCEPT:
Exfoliative cytology is indicated in which of the following situations?
Fine-needle aspiration cytology (FNAC) is contraindicated in which of the following conditions?
What is the recommended needle size for Fine Needle Aspiration Cytology (FNAC)?
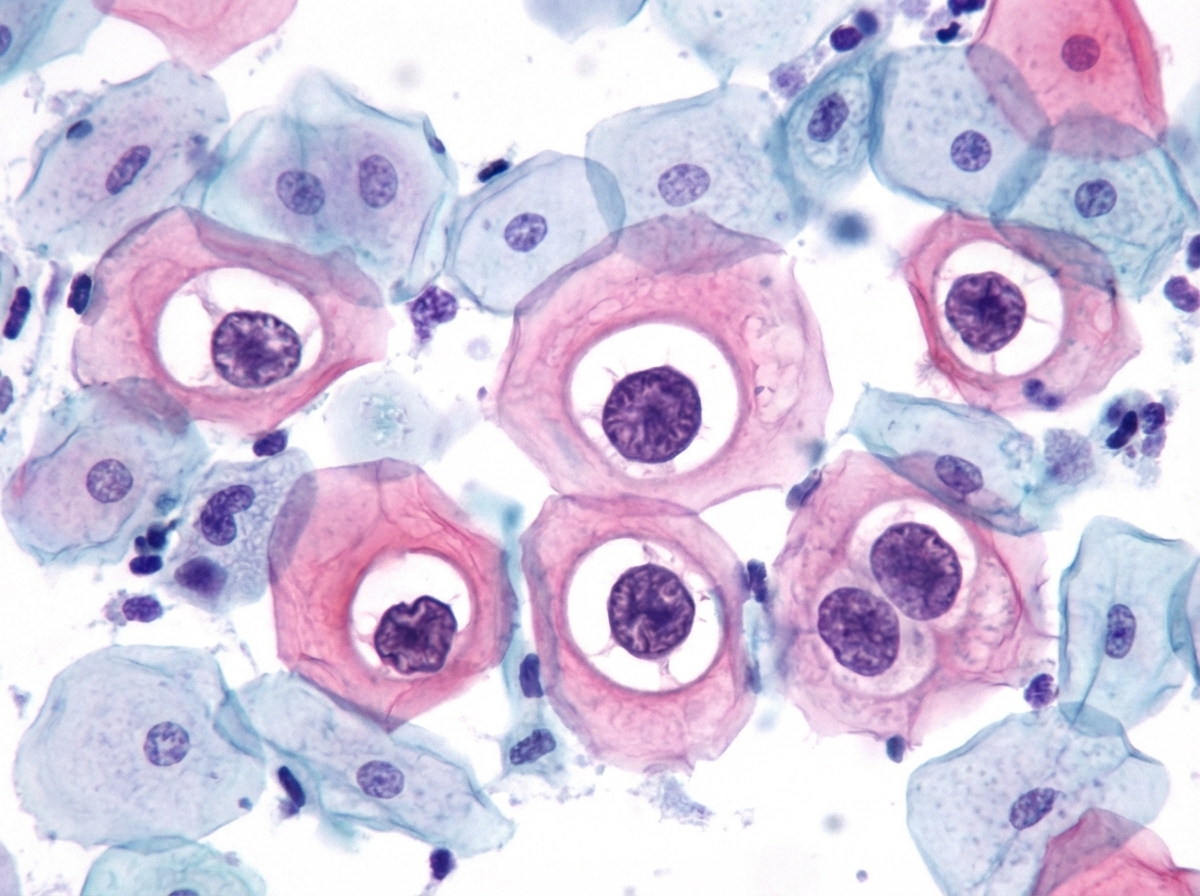
Based on the characteristic cytological findings on PAP smear examination in a 26-year-old female presented for screening, what is your diagnosis?
What is the best fixative for a Pap smear?
Regarding the screening of oral cancer, which of the following statements about exfoliative cytology is NOT true?
Vaginal cytology for hormonal assessment is best obtained from which location?
A maturation index of 100/0/0 indicates which of the following?
Fine needle aspiration cytology (FNAC) cannot detect which of the following conditions?
Practice by Chapter
Basic Principles of Cytopathology
Practice Questions
Specimen Collection and Processing
Practice Questions
Gynecologic Cytology
Practice Questions
Respiratory Tract Cytology
Practice Questions
Urinary Tract Cytology
Practice Questions
Effusion Cytology
Practice Questions
Fine Needle Aspiration Cytology
Practice Questions
Gastrointestinal Tract Cytology
Practice Questions
Ancillary Studies in Cytopathology
Practice Questions
Quality Assurance in Cytopathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app