
Cytopathology — MCQs

On this page
What is the commonly used gauge for Fine Needle Aspiration Cytology (FNAC) needles?
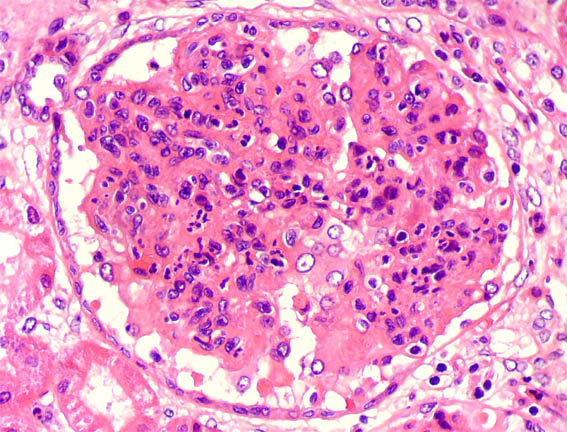
Examine the renal histopathology slide. What is the probable diagnosis?
For the diagnosis of carcinoma of the cervix, Pap smear screening is performed for what purpose?
In Pap smear cytology, which of the following is the most appropriate fixative used to preserve cellular details immediately after smearing?
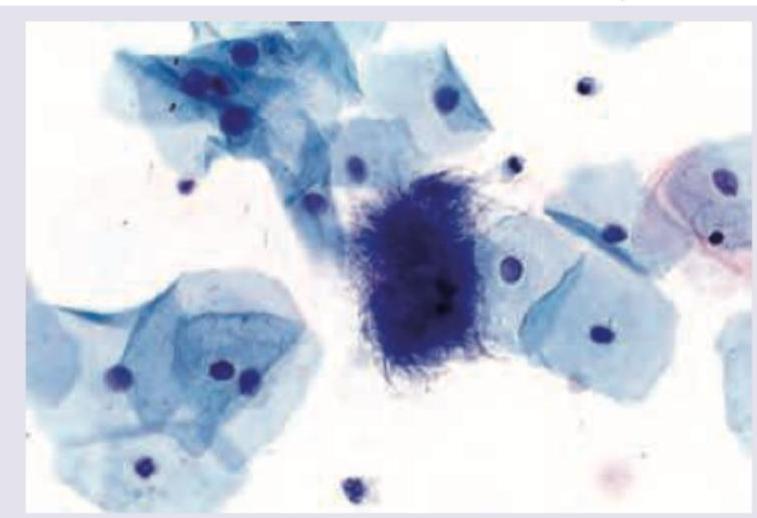
Name the cell shown in the Pap smear image.
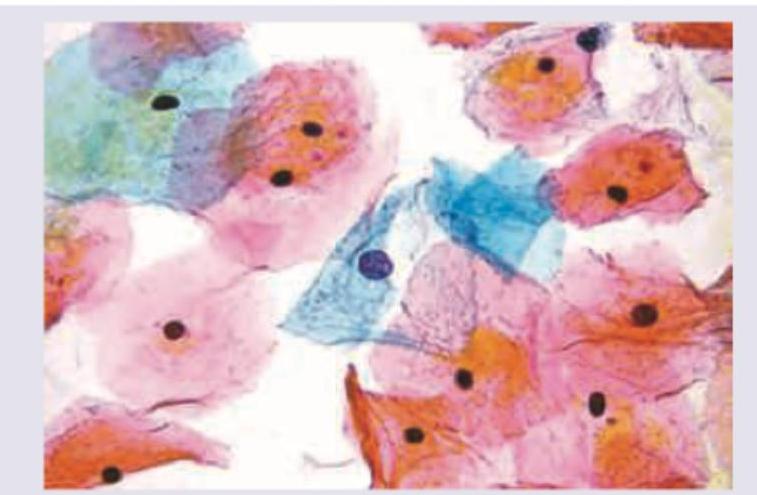
Name the cells marked as X in Pap smear.

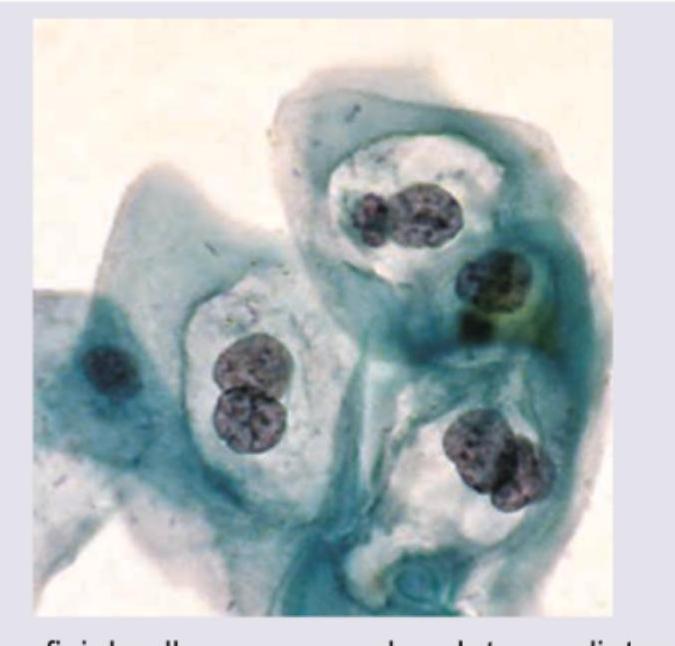
The following pap smear shows infestation by:
The following is the picture of the pap smear of a 45-year-old female with left ovarian tumor in her late menstrual phase showing squamous cells. What is the likely histology of the tumor?
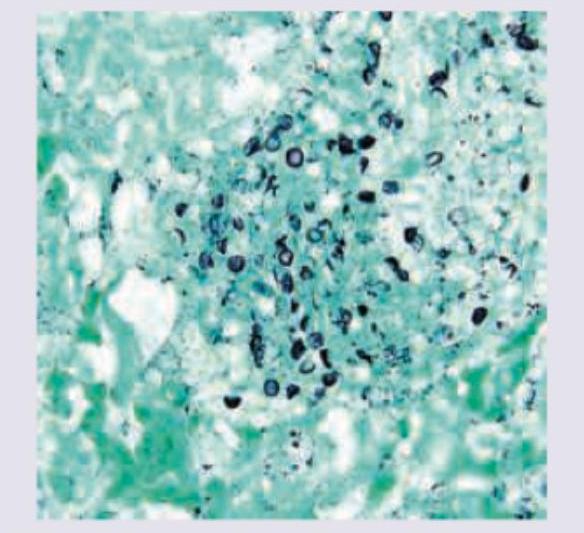
The following image of lung washing in AIDS positive patient is stained with:
Fine Needle Aspiration Cytology (FNAC) is NOT conclusive in which one of the following thyroid swellings?
Practice by Chapter
Basic Principles of Cytopathology
Practice Questions
Specimen Collection and Processing
Practice Questions
Gynecologic Cytology
Practice Questions
Respiratory Tract Cytology
Practice Questions
Urinary Tract Cytology
Practice Questions
Effusion Cytology
Practice Questions
Fine Needle Aspiration Cytology
Practice Questions
Gastrointestinal Tract Cytology
Practice Questions
Ancillary Studies in Cytopathology
Practice Questions
Quality Assurance in Cytopathology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app