
Cardiac Pathology — MCQs

On this page
Which of the following is NOT an effect of aging on the myocardium?
What is the characteristic pathological finding in carcinoid heart disease?
Concentric hypertrophy of the left ventricle is seen in which of the following conditions?
All are true about hyperopic obstructive cardiomyopathy except?
What is the most common site of myocardial infarction?
Irreversible changes in myocardial infarction are typically seen after how much time?
What is the most likely diagnosis in a patient presenting with large, friable, irregular vegetations on the heart valves?
Early granulation tissue in acute myocardial infarction is typically seen within which timeframe?
Myxoma commonly arises from which chamber of the heart?
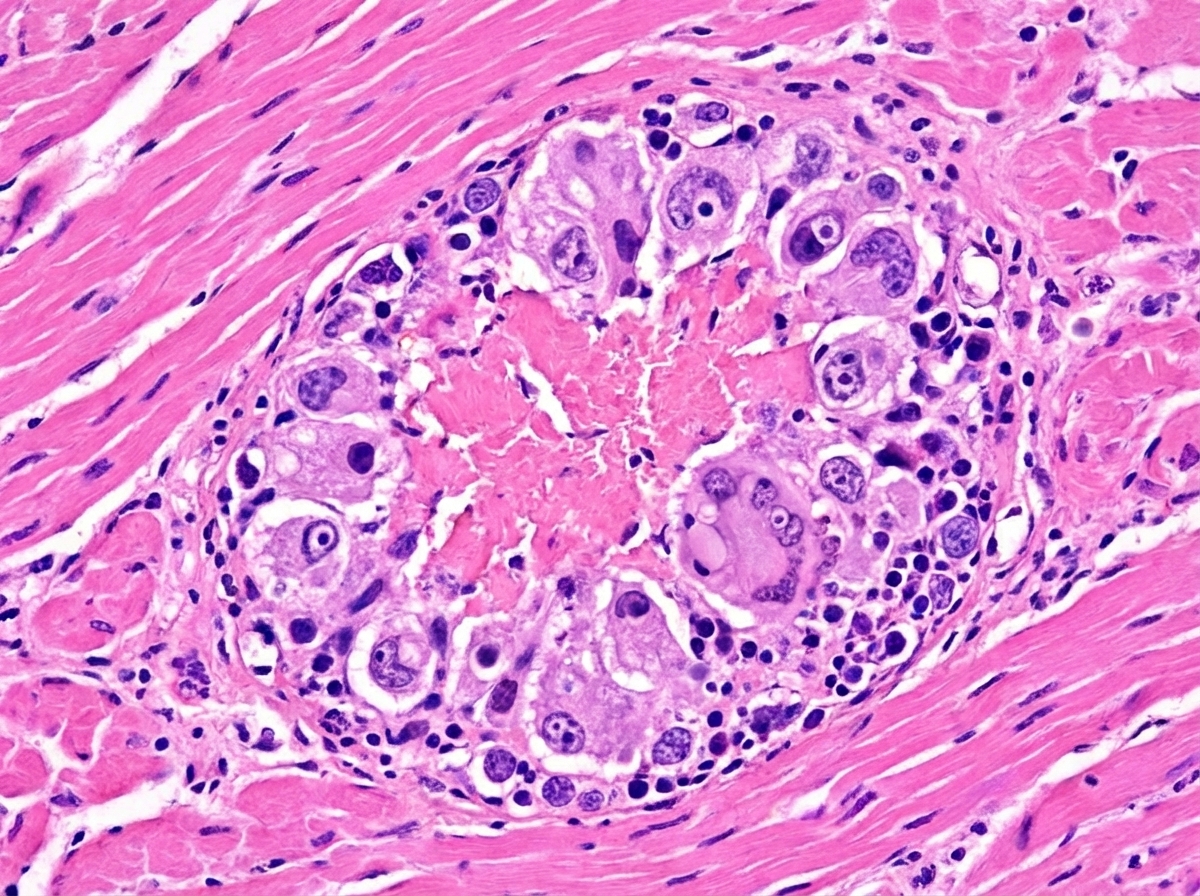
A 15-year-old boy presented with pancarditis. A myocardial biopsy showed a specific finding. What is the most likely histologic finding based on this image?
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app