
Cardiac Pathology — MCQs

On this page
Carcinoid of the heart presents as?
Which of the following is/are the characteristics of the vegetations seen in patients with Libman-Sacks endocarditis?
Vegetations on the under-surface of Aortic valve leaflets are typically found in which condition?
Which of the following forms of ischemic heart disease manifests with slowly progressive heart failure, with or without other clinical manifestations of myocardial ischemia?
Senile cardiac amyloidosis is due to deposition of amyloid which is similar to which of the following proteins?
A 15-year-old boy died suddenly while playing in the field. On autopsy, fibrofatty replacement of the right ventricular myocardium is seen. What is the most likely diagnosis?
Which is the most sensitive and specific marker for myocardial infarction?
A 25-year-old basketball player suddenly collapsed during an athletic event and died. Autopsy revealed a hypertrophied septum. What is the most probable diagnosis?
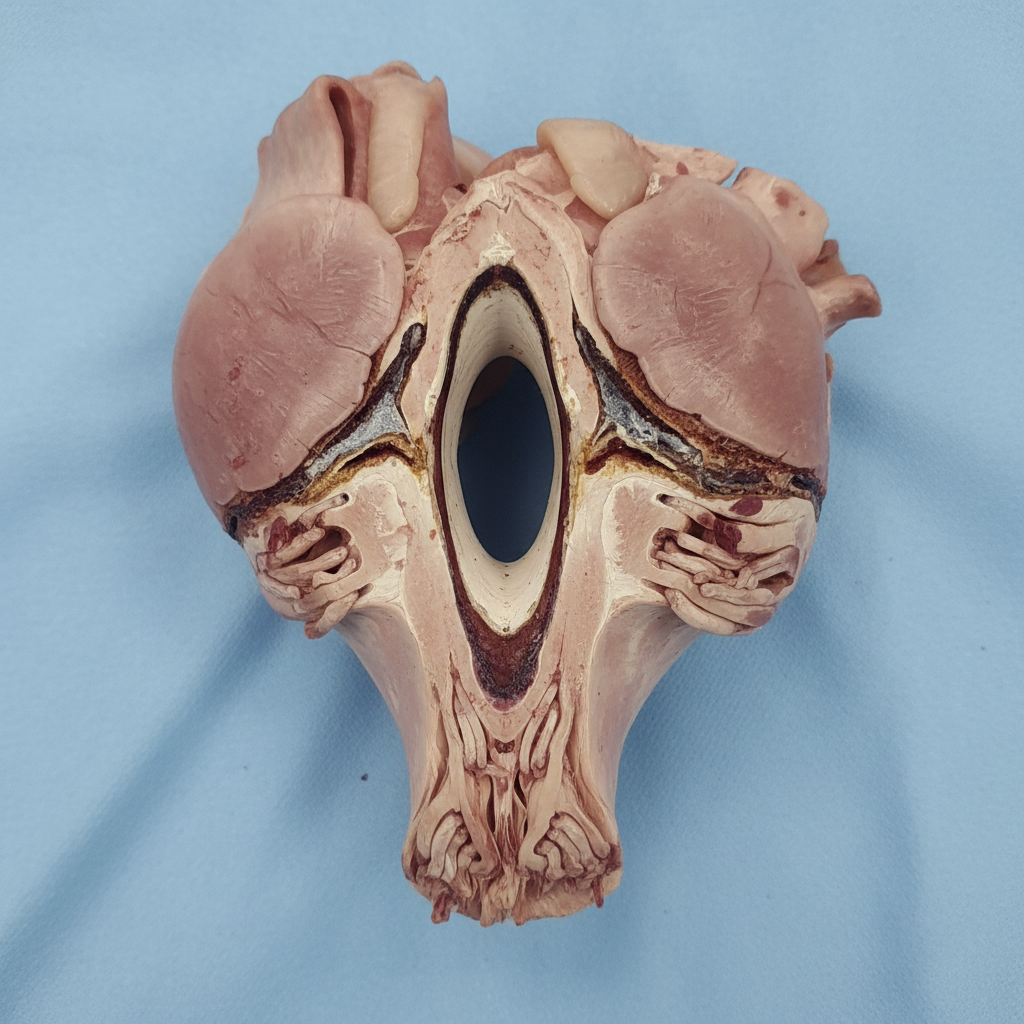
A 30-year-old male patient presented with dyspnea. Echocardiography showed mitral stenosis with left atrial hypertrophy. A gross specimen of the sectioned heart is shown in the image. What is the most likely diagnosis given the findings?
A patient with chest pain was diagnosed with myocardial infarction and received immediate thrombolytic therapy. Despite this, their cardiac condition worsened, leading to death. The patient was posthumously diagnosed with cardiac reperfusion injury. Which of the following histological findings is expected in the cardiac tissue following reperfusion injury?
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app