
Cardiac Pathology — MCQs

On this page
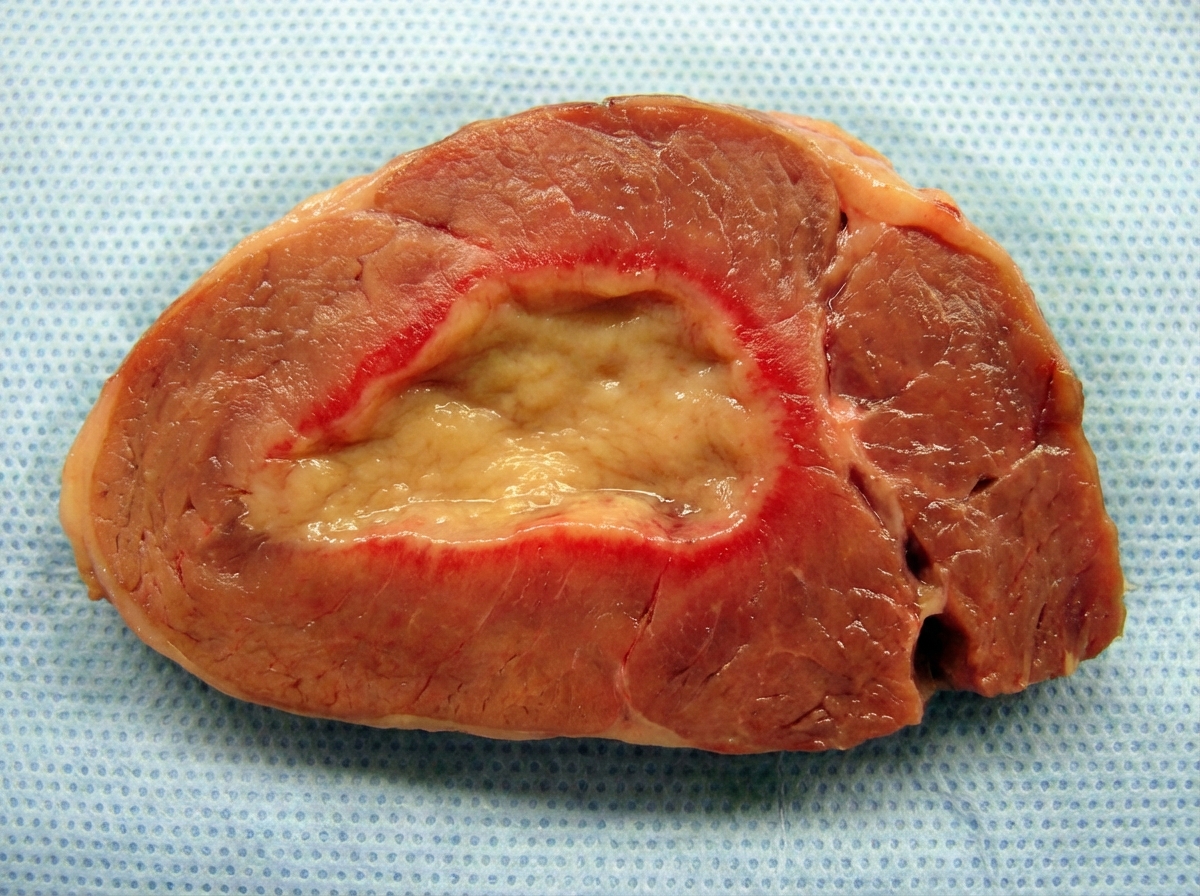
A gross section of the myocardium following myocardial infarction is shown. What is the likely duration following MI?
Which of the following is true of Rheumatic fever?
Calcification of the aortic valve is seen in which of the following conditions?
All are true about myxomas in the heart, EXCEPT:
A 73-year-old woman has had episodes of chest pain during the past week. She is afebrile. Her pulse is 80/min, respirations are 16/min, and blood pressure is 110/70 mm Hg. On auscultation of the chest, heart sounds seem distant, but the lung fields are clear. Neck veins are distended to the angle of the jaw, even while sitting. There is a darkly pigmented, irregular, 1.2-cm skin lesion on the right shoulder. A chest radiograph shows prominent borders on the left and right sides of the heart. Pericardiocentesis yields bloody fluid. Laboratory findings include a serum troponin I level of 0.3 ng/mL. Which of the following lesions is the most likely cause of these findings?
Which of the following findings is expected on microscopic examination of a biopsy from a heart showing ventricular hypertrophy with asymmetric septal thickening?
A 62-year-old woman undergoing chemotherapy for breast cancer presents with a 3-day history of fever and chest pain. Cardiac catheterization reveals a markedly reduced ejection fraction with normal coronary blood flow. A myocardial biopsy is obtained, and a PCR test for coxsackievirus is positive. Histologic examination of this patient's myocardium will most likely reveal an abundance of which of the following inflammatory cells?
A 4-year-old boy with a history of intellectual disability and seizures presents with a one-month history of shortness of breath. Physical examination reveals numerous papules on the face. Echocardiography shows tumor-like growth in the left ventricle. What is the most likely diagnosis for this patient's condition?
Concentric hypertrophy of the heart is most commonly associated with which of the following conditions?
What is true about vegetations in rheumatic fever?
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app