
Cardiac Pathology — MCQs

On this page
What is the most characteristic histological finding of acute rheumatic carditis?
Carcinoid heart disease affects which part of the heart?
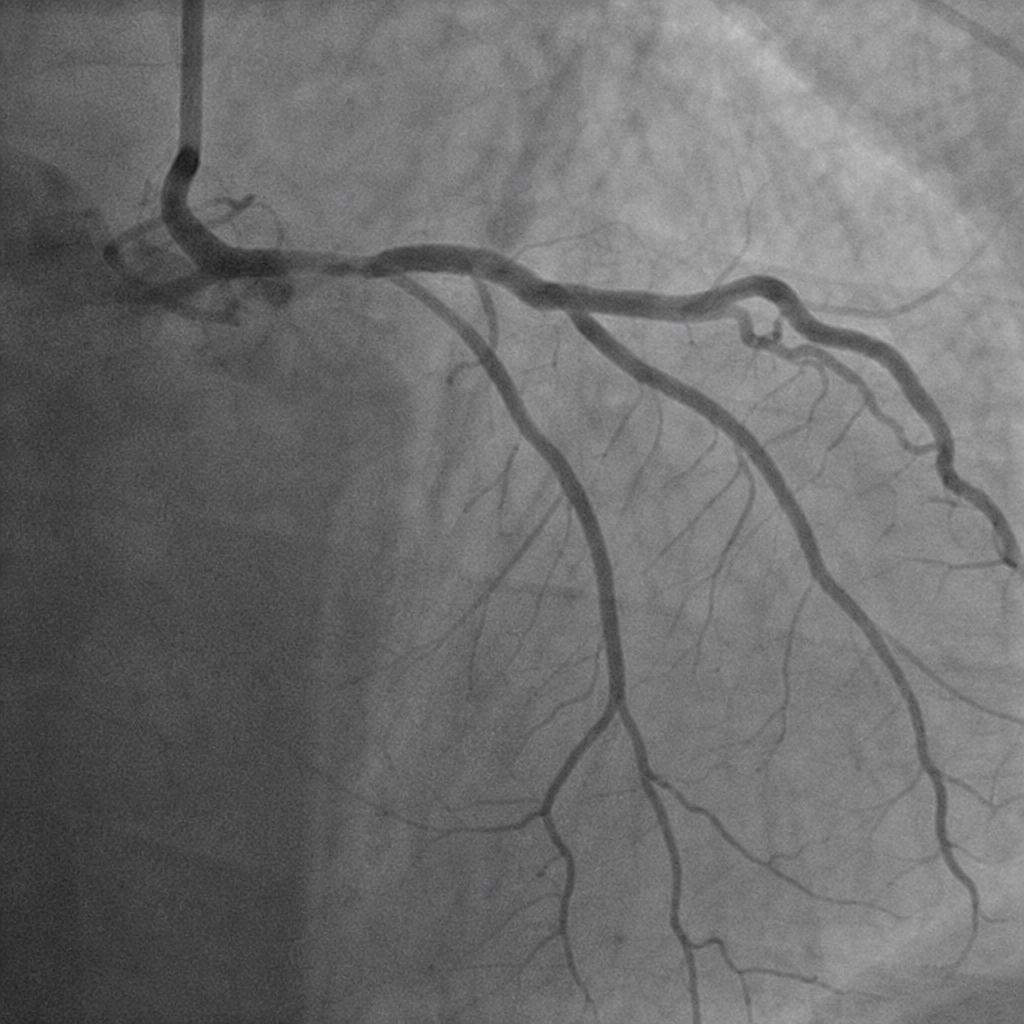
Which coronary artery is occluded?
A 60-year-old man has had angina on exertion for the past 6 years. A coronary angiogram performed 2 years ago showed 75% stenosis of the left circumflex coronary artery and 50% stenosis of the right coronary artery. For the past 3 weeks, the frequency and severity of his anginal attacks have increased, and pain sometimes occurs even when he is lying in bed. On physical examination, his blood pressure is 110/80 mm Hg, and pulse is 85/min with irregular beats. An ECG shows ST-segment elevation. Laboratory studies show serum glucose, 188 mg/dL; creatinine, 1.2 mg/dL; and troponin I, 1.5 ng/mL. Which of the following is most likely to explain these findings?
Rheumatic heart disease is caused by all of the following except?
In myocardial infarction, fibrosis is typically seen after how many days?
A patient with long-standing, moderately severe anemia dies in an automobile accident. An autopsy is performed. Which of the following cardiac changes will MOST likely be seen when the heart is examined?
What is the most common benign heart tumor?
Rupture of the myocardium typically occurs within what time frame after a myocardial infarction?
Which of the following vessels is most commonly affected by atherosclerosis?
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app