
Cardiac Pathology — MCQs

On this page
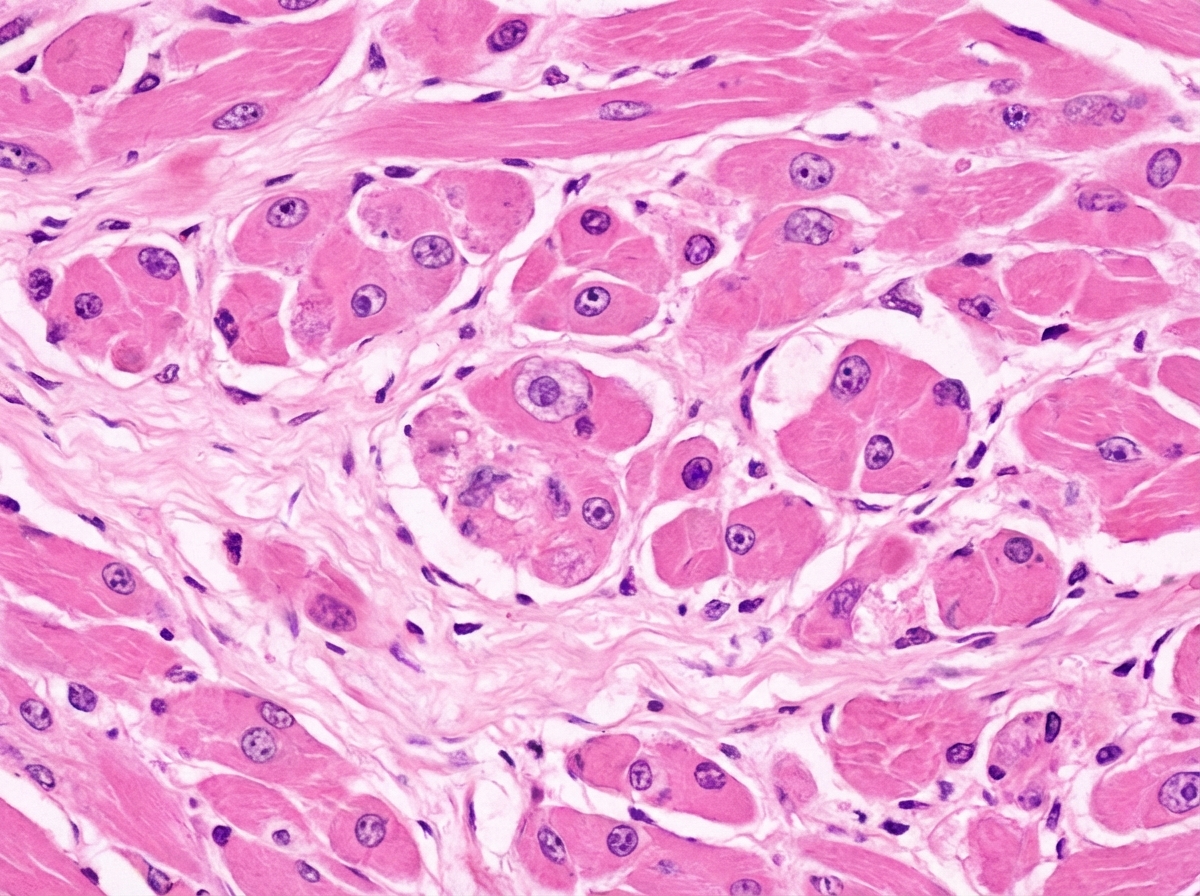
A 25-year-old bodybuilder was using anabolic steroids and started having puffy feet for the last 2 months. He died suddenly during a workout. Post-mortem examination revealed dilated ventricular chambers with reduced systolic function. A post-mortem heart biopsy specimen is shown below. What is the diagnosis?
What is the most common tumor of the heart?
Carcinoid of the heart typically involves which structure?
A 29-year-old male athlete suddenly collapsed and died during a football game. Autopsy revealed a specific gross examination finding. He had a history of two similar deaths in the family. What is the most likely cause of death?

Dilated cardiomyopathy is due to which of the following?
Which of the following dissection methods of the heart is most useful for demonstrating the distribution of infarction?
A 50-year-old woman presents with fatigue and shortness of breath. Physical examination shows evidence of pulmonary edema, enlargement of the left atrium, and calcification of the mitral valve. A CT scan demonstrates a large obstructing mass in the left atrium. Before open heart surgery can be performed to remove the tumor, the patient suffers a stroke and expires. Which of the following hemodynamic disorders best explains the pathogenesis of stroke in this patient?
A four-month-old child develops cardiac failure and dies three months later. At autopsy, the heart has no obvious congenital defects, but the cardiac chambers are small and covered with thick, white endocardium. Histological sections of the heart demonstrate regular bands of elastic tissue in the thick fibrous endocardium. Which of the following is the most likely diagnosis?
Which of the following is the commonest cardiac neoplasm in adults?
Left ventricular hypertrophy is caused by all EXCEPT?
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app