
Cardiac Pathology — MCQs

On this page
Anitschkow cells are?
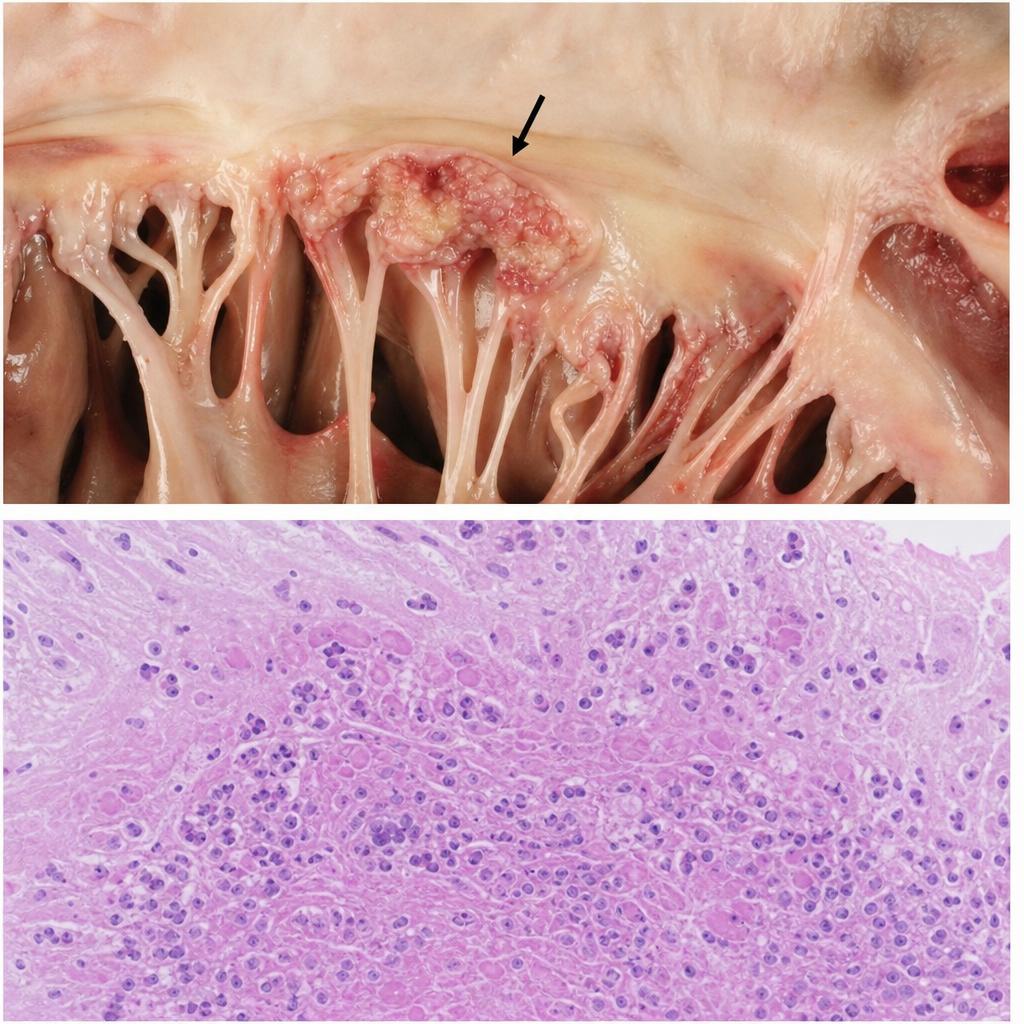
Which condition causes large friable destructive vegetations containing microorganisms and inflammatory cells on the mitral valve?
Which of the following will be seen on cardiac biopsy of a patient who had a post MI reperfusion injury?
Fish mouth appearance of valve in RHD is due to-
Most common malignant tumor of the heart in adults
Aetiology of Dressler Syndrome is
What type of necrosis is associated with Myocardial Infarction (MI)?
Which type of white blood cell plays a primary role in cardiac remodeling and chronic inflammation in heart failure?
Concentric hypertrophy of left ventricle is seen in -
Which protein is defective in dilated cardiomyopathy?
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app