
Cardiac Pathology — MCQs

On this page
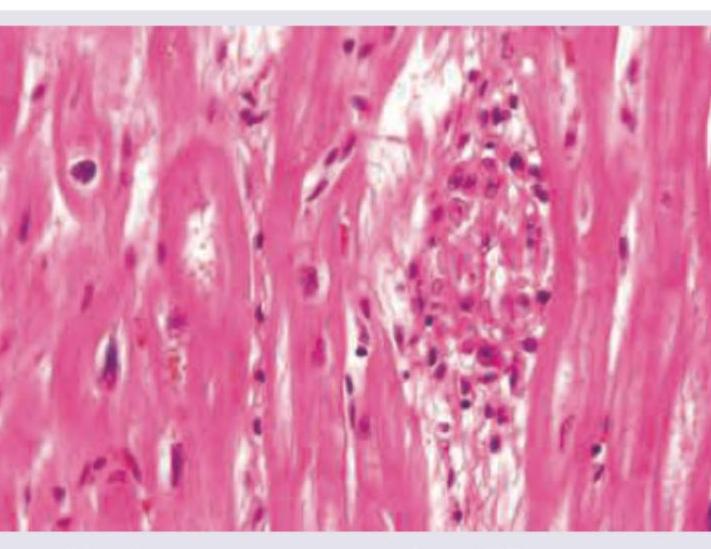
An 18-year-old male with severe effort intolerance and dyspnea is found to have left atrial enlargement on Chest X-ray. He also has features of active rheumatic carditis. Histopathological examination shows:
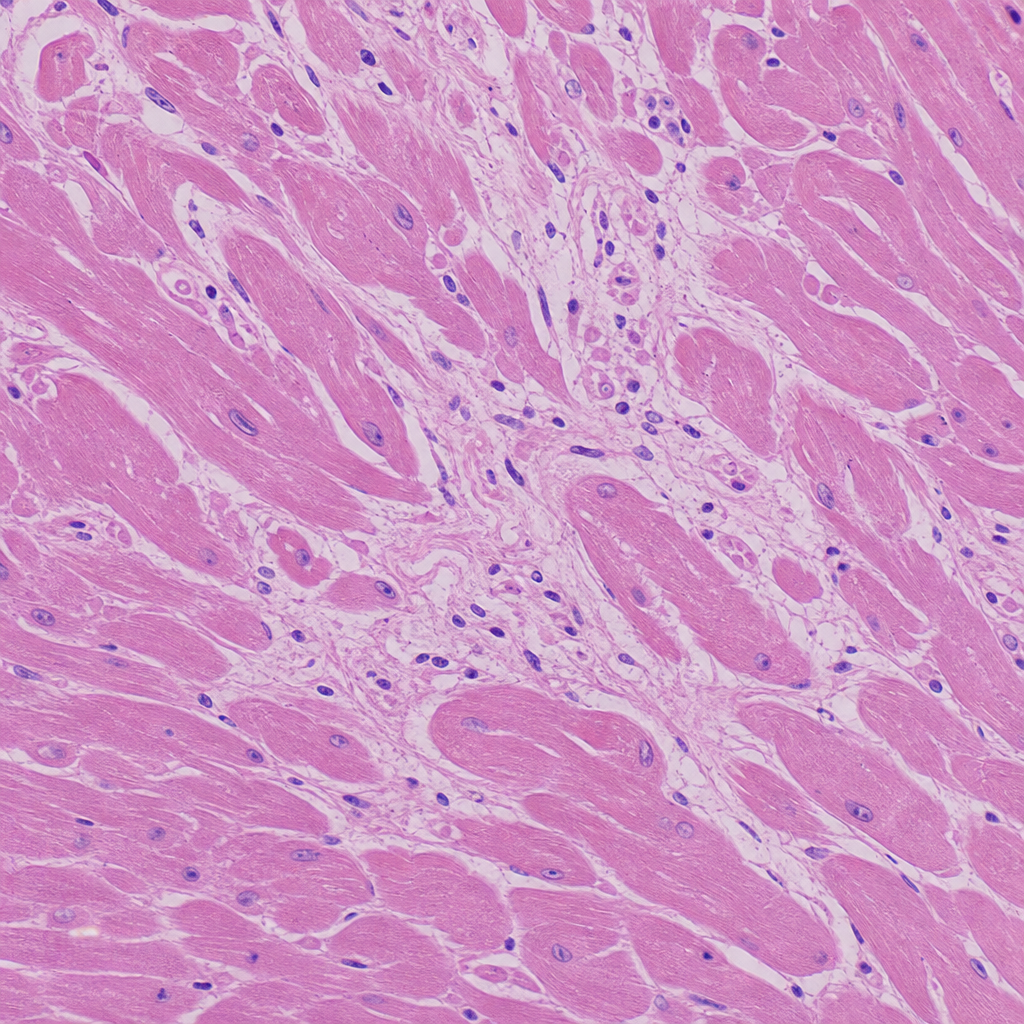
A 30-year-old football player presented to the emergency department with sudden cardiac arrest/collapse. Based on the histological image provided, what is the most likely cause of his death?
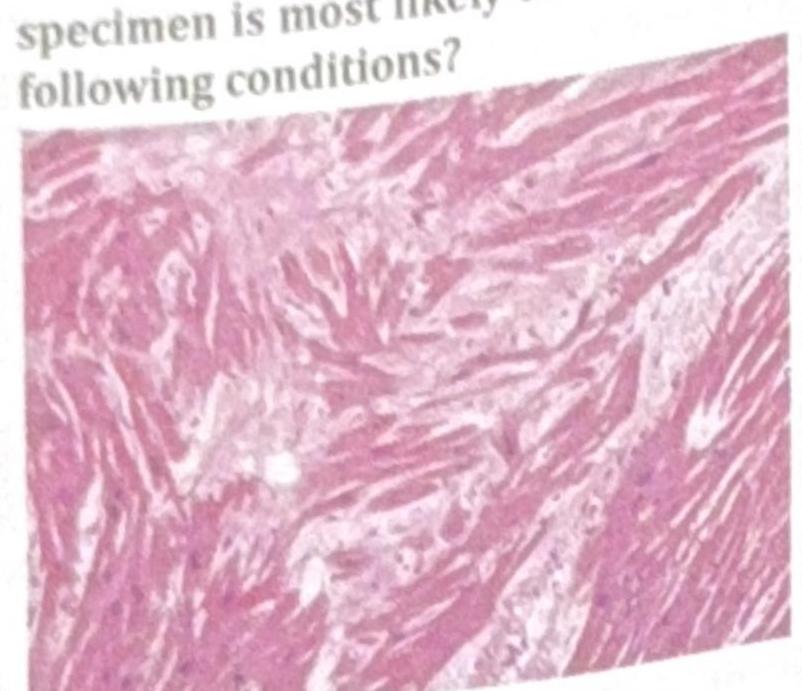
An athlete collapsed and expired while playing school basketball. Histology of the cardiac specimen is most likely to indicate which of the following conditions?
What is the histopathological finding 12 hours after ischemic injury to heart?
Which of the following has the most friable vegetations:
In rheumatic heart disease, infective endocarditis is detected by echocardiogram and the largest vegetations seen are due to -
Vegetations on under surface of cusps are found in:
All of the following arteries are common sites of occlusion by a thrombus except:
A patient presents with acute rheumatic carditis with fever. The true statement is:
Features of rheumatic carditis are all except:
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app