
Cardiac Pathology — MCQs

On this page
A 65-year-old man dies due to myocardial infarction. Which stains can be used to see the infarct in the heart while conducting an autopsy?
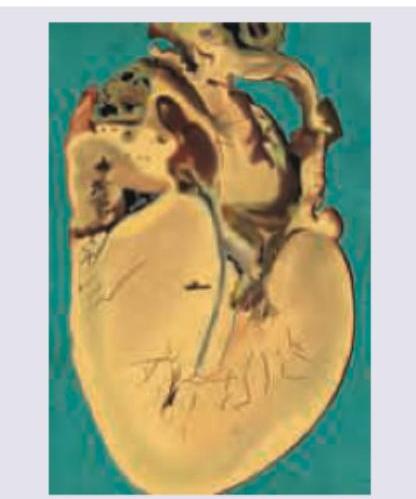
An athlete collapsed suddenly during exercise and died on the field. Postmortem heart is shown in the figure. There is family history of heart disease. What is the diagnosis?
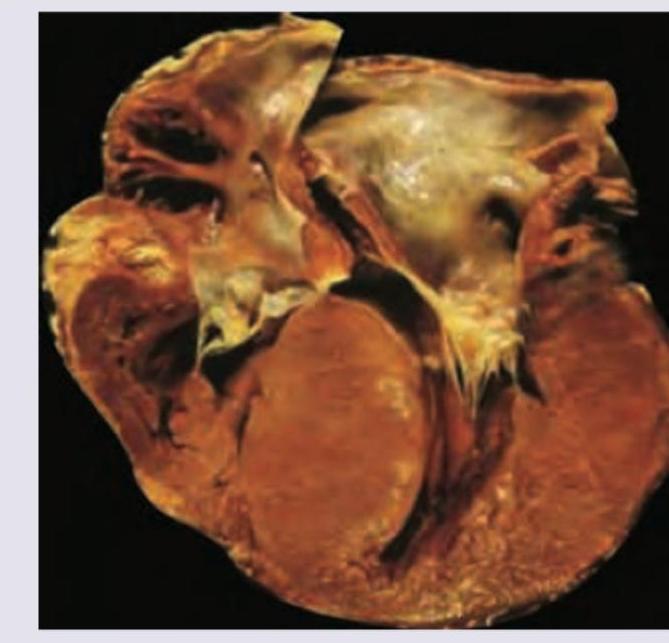
All are true regarding the heart specimen shown (classic asymmetric septal obstructive form of HCM) except:
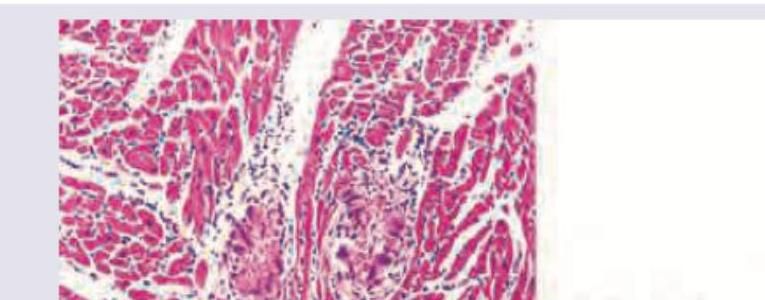
A patient with a history of rheumatic fever presents with cardiac symptoms. Identify the diagnosis from the myocardial histopathology depicted below. (AIIMS Nov 2017)
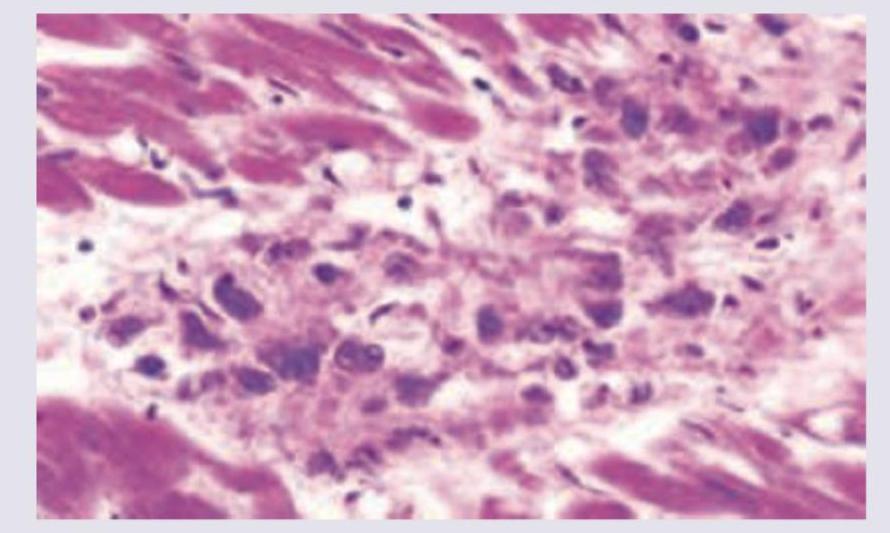
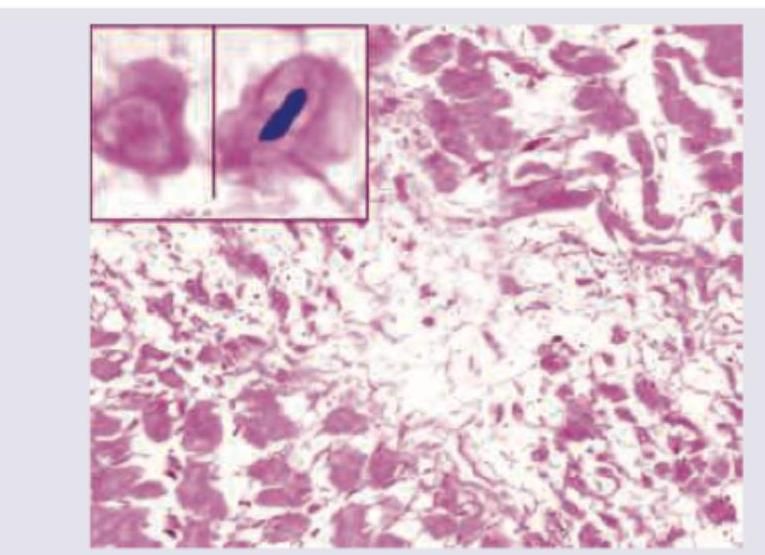
A 5-year-old child presents with fever and chest pain 3 weeks after a sore throat. On auscultation, pericardial friction rub was heard with bilaterally clear lung fields. A myocardial biopsy is performed. The Histopathological finding shows presence of:
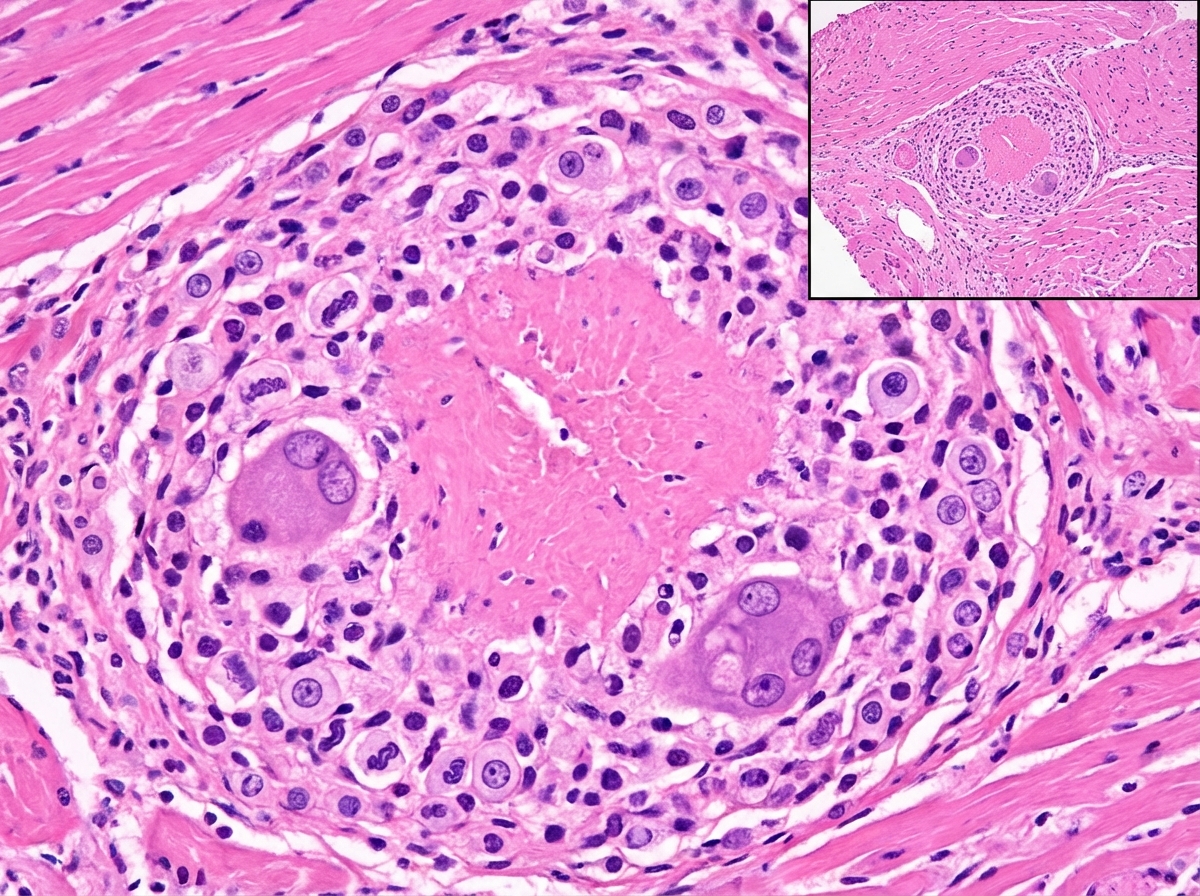
Which of the following is the most common cause of death in this condition?
The following image shows presence of:
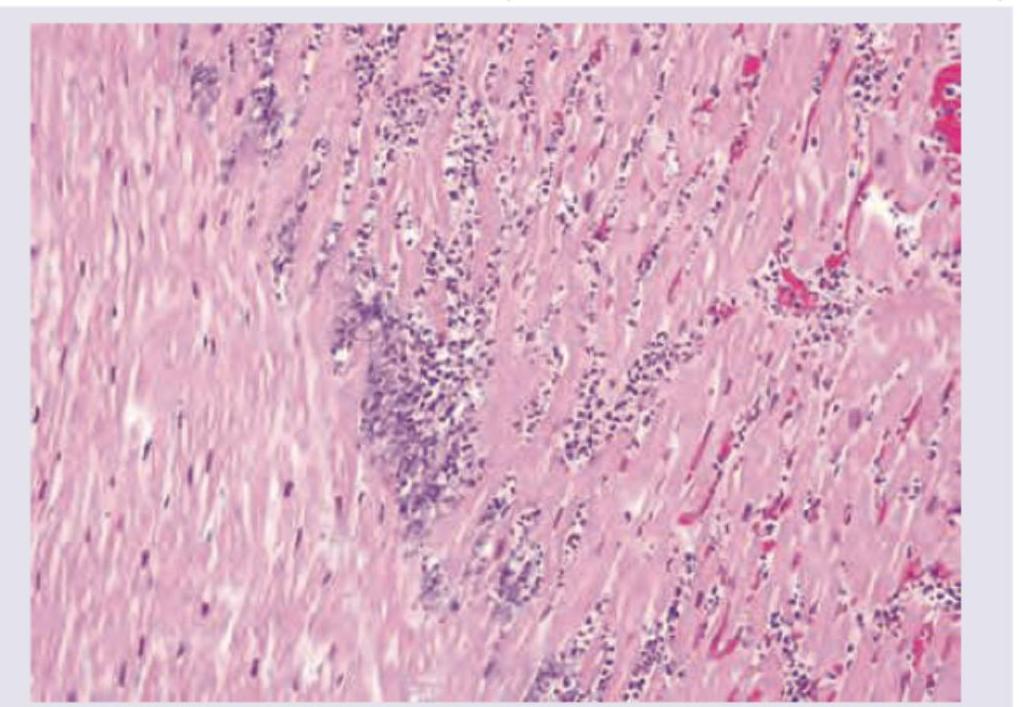
The image shows infarcted tissue of the heart that develops after
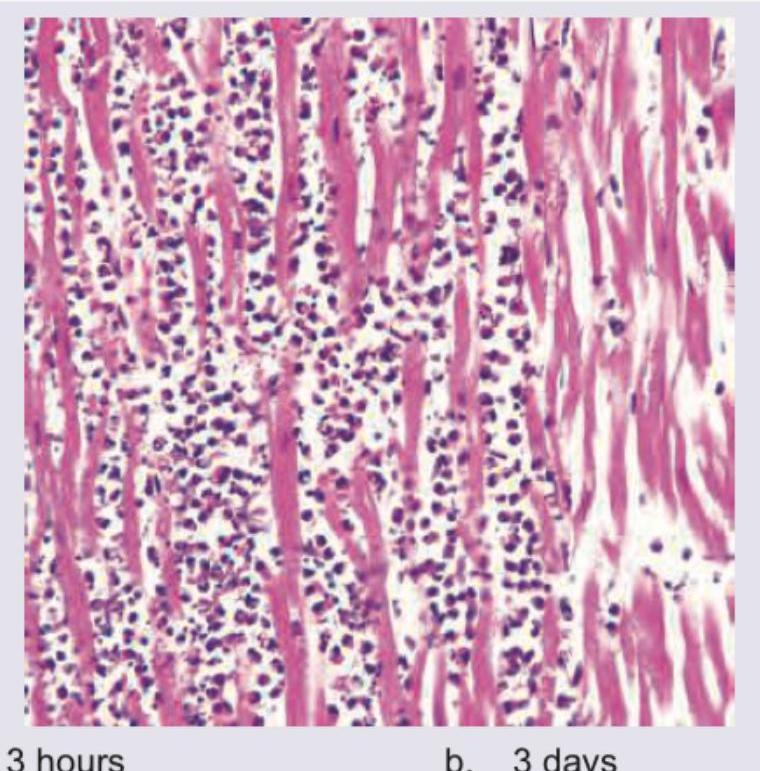
The following is the Hematoxylin and Eosin stained section from the heart of a patient after myocardial infarction. What can you say about the age of the infarction?
In a patient, Mitral valve vegetations are seen along the lines of closure along with fusion of commissures. What is the likely diagnosis?

Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app