
Cardiac Pathology — MCQs

On this page
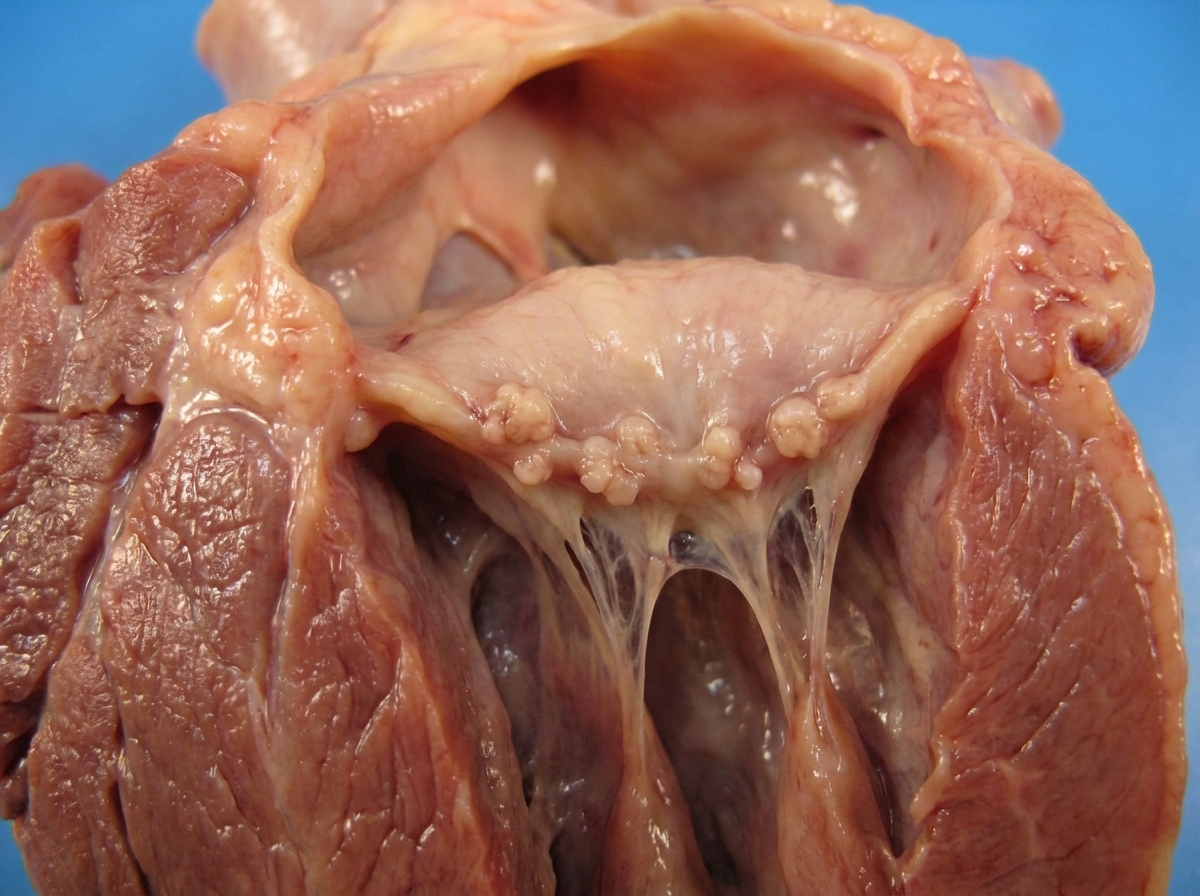
Gross findings of the heart from an 18-year-old female presented with a history of sore throat 3 months back and joint pains have been shown below. On auscultatory finding, a murmur was noted. What is your diagnosis?
A 41-year-old woman presents with a week of increasing dyspnea. Physical examination reveals a temperature of 37.3°C, pulse of 85/min, respirations of 20/min, and blood pressure of 150/95 mm Hg. There is dullness to percussion over the lung bases. A chest radiograph shows large bilateral pleural effusions and a normal heart size. Laboratory findings include serum creatinine of 3.1 mg/dL, urea nitrogen of 29 mg/dL, troponin I of 0.1 ng/mL, WBC count of 3760/mm³, hemoglobin of 11.7 g/dL, and positive ANA and anti-double-stranded DNA antibody test results. Which of the following cardiac lesions is most likely to be present in this patient?
A man dies 5 days after suffering a myocardial infarction. What will a myocardial biopsy show?
A 36-year-old man with a history of long-standing rheumatic heart disease and mitral stenosis dies during cardiac surgery. Autopsy findings are consistent with mitral stenosis and reveal the presence of "heart failure cells." What process leads to the observation of "heart failure cells"?
At the time of autopsy of a 39-year-old female who died of complications of systemic lupus erythematosus, several medium-sized vegetations are found on both sides of the mitral valve and tricuspid valve. These cardiac vegetations are most likely the result of?
Ground glass appearance of the ventricular septum is seen in which of the following conditions?
Which of the following statements is NOT true regarding the specimen shown?

Antischkow cells are seen in all conditions EXCEPT:
In patients with hypertrophic cardiomyopathy, in which gene are the maximum mutations found?
Which carcinoma metastasizes to the heart?
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app