
Cardiac Pathology — MCQs

On this page
Histopathological examination of cardiac tissue from a post-MI patient shows a predominant neutrophilic infiltrate. This finding corresponds to which post-infarction time window?
A 35-year-old woman from a low socioeconomic background presents with progressive exertional dyspnoea, orthopnoea, and haemoptysis. She gives a history of recurrent sore throats in childhood. Auscultation reveals a mid-diastolic rumble at the apex. The gross pathology specimen of the explanted valve is shown in Image 2. Which of the following pathological mechanisms is most directly responsible for the valvular deformity seen in this image?

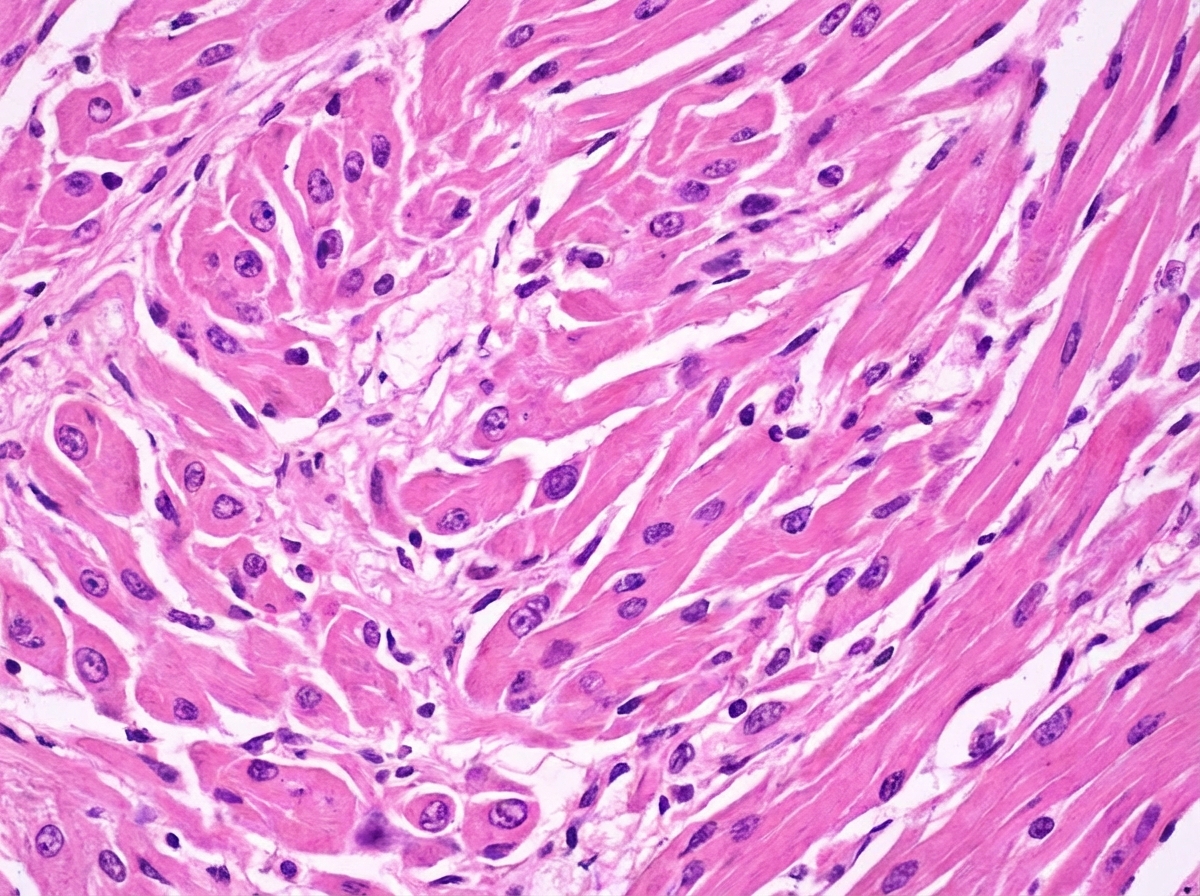
What type of cardiomyopathy is characterized by this arrangement of myofibrils?
What is the mechanism of acute rheumatic fever?
What is the typical site of lesion in endocarditis of rheumatic heart disease?
Practice by Chapter
Congenital Heart Disease
Practice Questions
Ischemic Heart Disease
Practice Questions
Hypertensive Heart Disease
Practice Questions
Valvular Heart Disease
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Pericardial Disease
Practice Questions
Cardiac Tumors
Practice Questions
Heart Failure Pathophysiology
Practice Questions
Cardiac Transplantation Pathology
Practice Questions
Endocarditis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app