
Bone and Soft Tissue Pathology — MCQs

On this page
Narrow, high arched palate, prolonged retention of deciduous teeth, and failure in the eruption of permanent teeth are characteristic of which condition?
Osteoid osteoma consists of:
What is a common complication seen in a patient with osteopetrosis during tooth extraction?
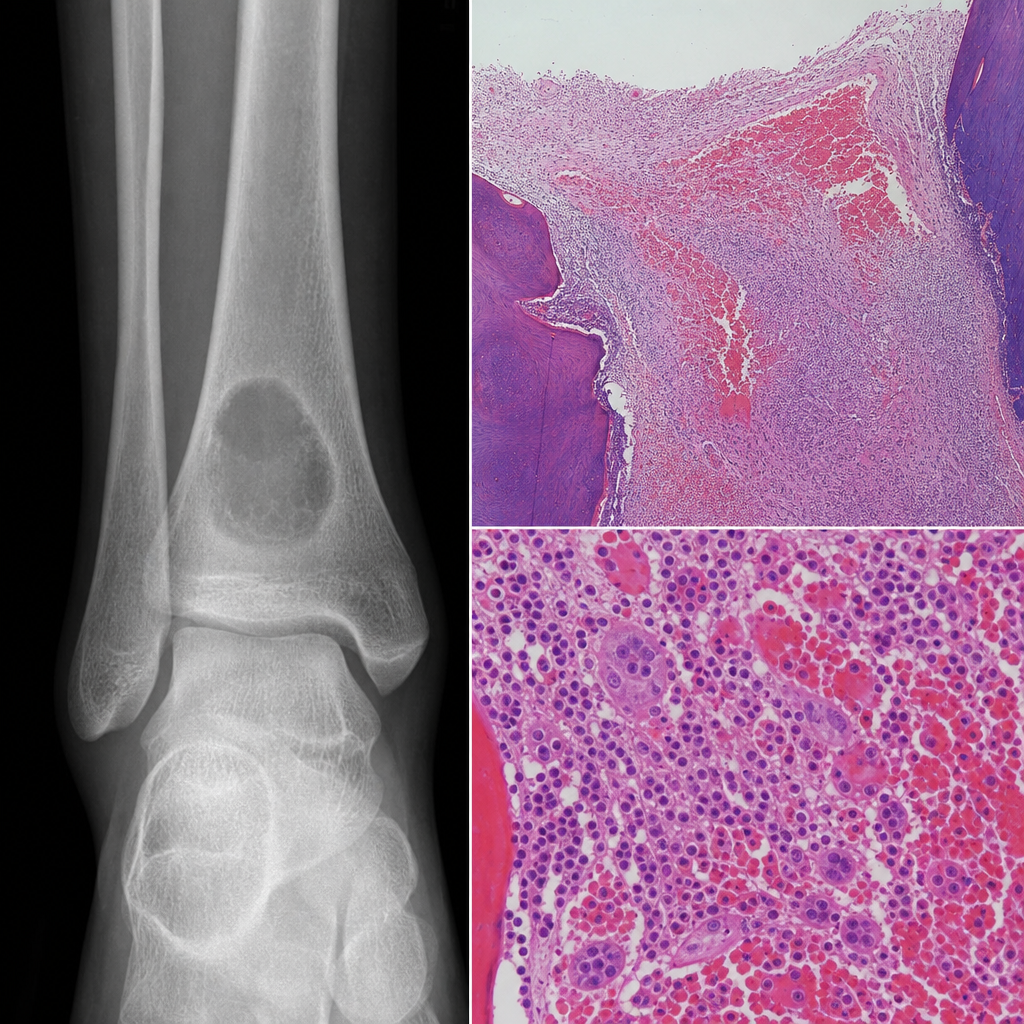
A patient with known severe hemophilia A (deficient Factor VIII activity) and a history of recurrent bleeding episodes presented with pain in his ankle. X-ray shows an osteolytic lesion with a sclerotic rim. Histopathological findings are available. What is your diagnosis?
Which of the following periapical conditions is often associated with a vital pulp?
A 50-year-old patient presents with a midline lesion involving the sacrum, which is found to be sclerotic. What is the most probable diagnosis?
Following a fracture of the humerus, a biopsy of the healing area of an adult patient is performed. Which of the following types of bone will the biopsy most likely show?
Which of the following is false regarding Cherubism?
Which of the following statements about embryonal rhabdomyosarcoma is false?
All of the following are examples of round cell tumors except?
Practice by Chapter
Bone Development and Growth
Practice Questions
Fracture Healing
Practice Questions
Osteomyelitis and Infectious Diseases
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone Tumors and Tumor-like Lesions
Practice Questions
Joints and Rheumatologic Diseases
Practice Questions
Soft Tissue Tumors
Practice Questions
Muscular Dystrophies and Myopathies
Practice Questions
Diseases of Tendons and Fascia
Practice Questions
Pathology of Orthopedic Implants
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app