
Bone and Soft Tissue Pathology — MCQs

On this page
A 30-year-old male presents with swelling around the knee joint. Histopathological examination reveals many giant cells interspersed with mononuclear cells. What is the most likely diagnosis?
Chordoma arises from:
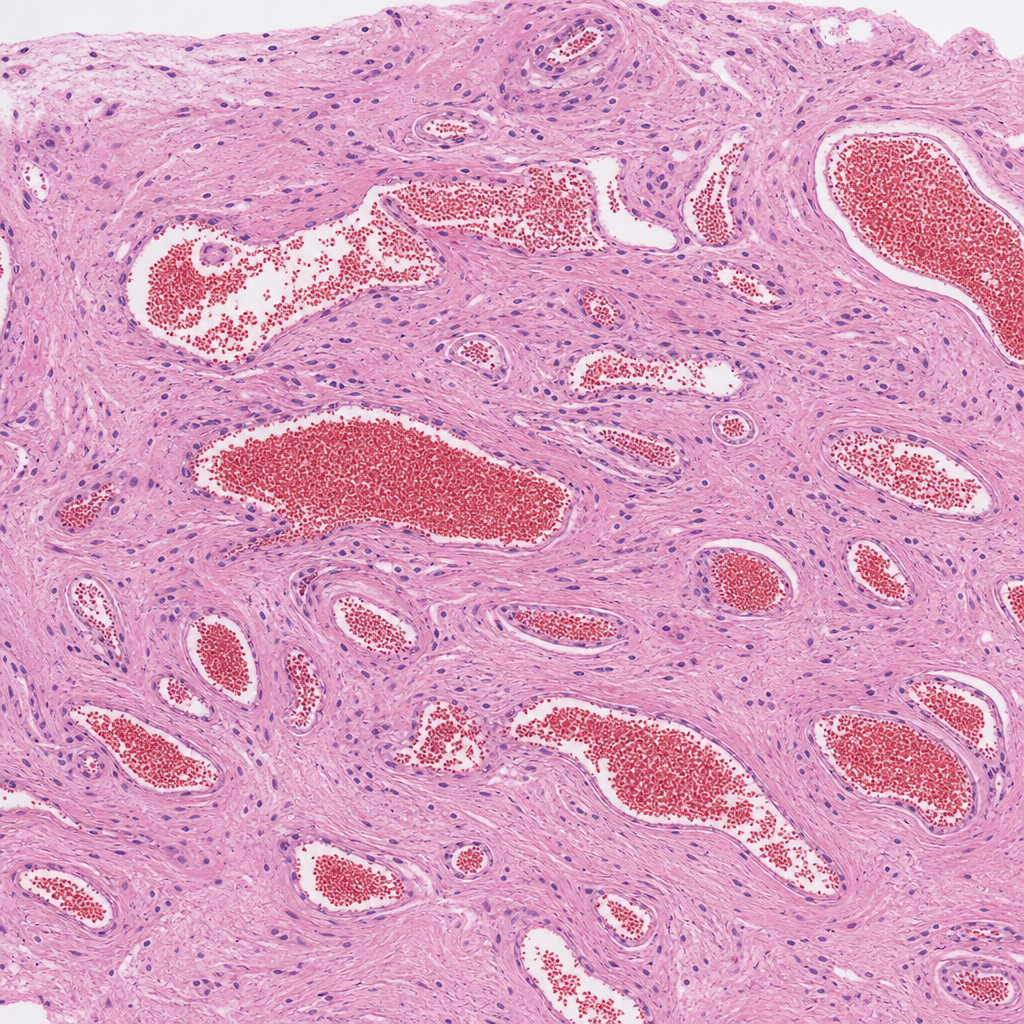
A red soft to firm swelling on the sternum that on biopsy shows the following histology. An image is provided for diagnosis. What is the diagnosis?
All of the following are true regarding Paget's Disease except which of the following?
All are features of Paget's disease except which of the following?
Which of the following is commonly associated with osteolytic metastasis?
What is the most common malignant tumor of the skeletal system?
Which of the following statements about chronic osteomyelitis is false?
Brown tumors are seen in:
What are the common causes of vertebra plana?
Practice by Chapter
Bone Development and Growth
Practice Questions
Fracture Healing
Practice Questions
Osteomyelitis and Infectious Diseases
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone Tumors and Tumor-like Lesions
Practice Questions
Joints and Rheumatologic Diseases
Practice Questions
Soft Tissue Tumors
Practice Questions
Muscular Dystrophies and Myopathies
Practice Questions
Diseases of Tendons and Fascia
Practice Questions
Pathology of Orthopedic Implants
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app