
Bone and Soft Tissue Pathology — MCQs

On this page
Identify the lesion in a 20-year-old male whose foot X-ray is shown below:
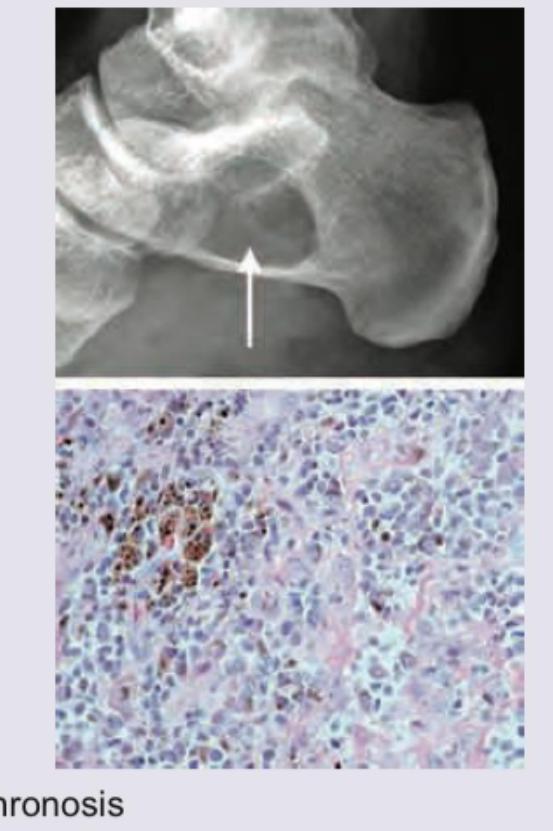
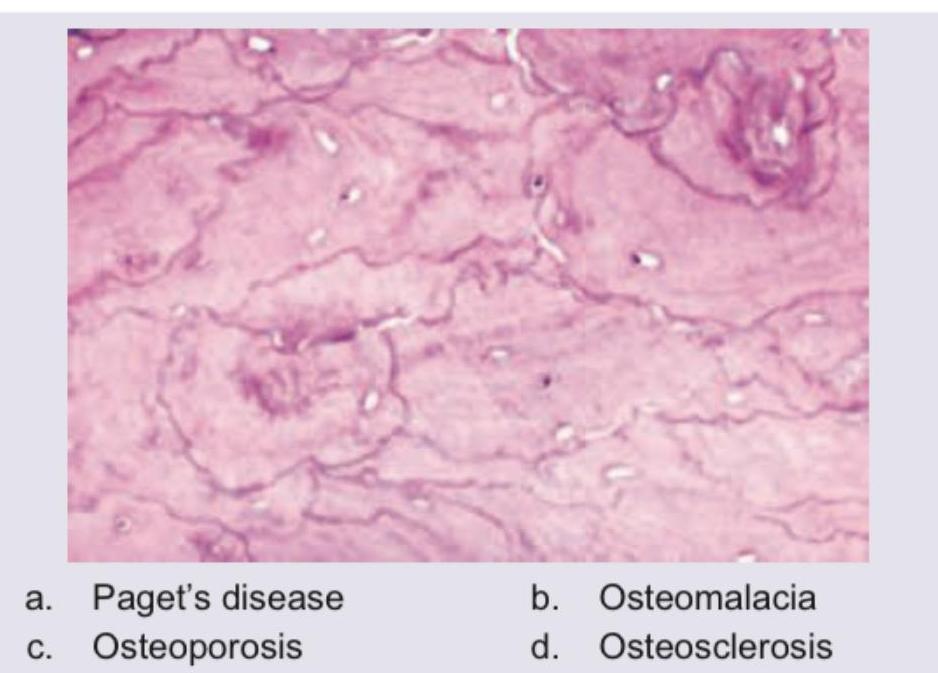
Bone biopsy specimen is shown below. Diagnosis is:
A 5 year old child who presented with proptosis of one of the eyes was found to have a desmin positive tumour. What is the probable diagnosis?
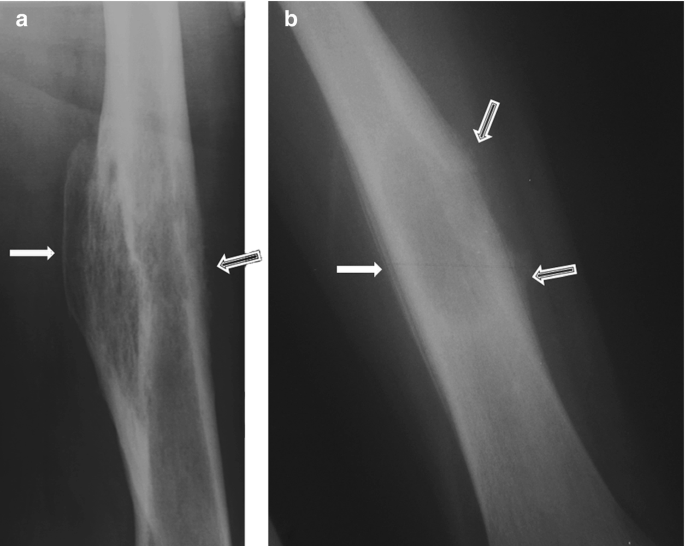
A 12-year-old Caucasian male presents with his mother to the pediatrician’s office complaining of right thigh pain. He reports that he has noticed slowly progressive pain and swelling over the distal aspect of his right thigh over the past two months. He denies any recent trauma to the area and his temperature is 100.9°F (38.3°C). On exam, there is swelling and tenderness overlying the distal right femoral diaphysis. Laboratory evaluation is notable for an elevated white blood cell (WBC) count and elevated erythrocyte sedimentation rate (ESR). A radiograph of the patient’s right leg is shown. Biopsy of the lesion demonstrates sheets of monotonous small round blue cells with minimal cytoplasm. Which of the following genetic mutations is most likely associated with this patient’s condition?
A muscle biopsy shows 'moth-eaten' fibers. Which histochemical finding would confirm mitochondrial myopathy?
Albers-Schönberg disease is:
Marble bone disease is:
Crystals deposited in Pseudogout:
Osteogenesis imperfecta is due to
Mutations in type I collagen fibres results in:
Practice by Chapter
Bone Development and Growth
Practice Questions
Fracture Healing
Practice Questions
Osteomyelitis and Infectious Diseases
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone Tumors and Tumor-like Lesions
Practice Questions
Joints and Rheumatologic Diseases
Practice Questions
Soft Tissue Tumors
Practice Questions
Muscular Dystrophies and Myopathies
Practice Questions
Diseases of Tendons and Fascia
Practice Questions
Pathology of Orthopedic Implants
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app